Acute lymphocytic leukemia (ALL)
|
|
 PubMed abstracts: Review | Therapy | Diagnosis PubMed abstracts: Review | Therapy | Diagnosis
|
Acute Lymphocytic
Leukemia (ALL)
Also see Childhood Lymphoma
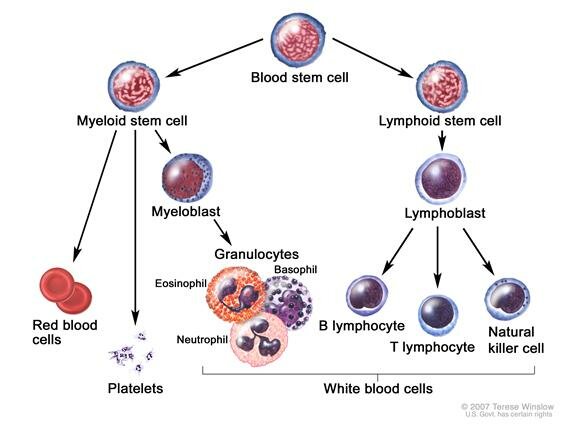
B-cell stage: stem cell
|
"ALL is the most common cancer occurring in children, representing 23% of cancer diagnoses among children younger than 15 years of age and occurring at an annual rate of approximately 31 per million. There are approximately 2,400 children and adolescents younger than 20 years of age diagnosed with ALL each year in the United States.
There is a sharp peak in ALL incidence among children ages 2 to 3 years (> 80 per million per year), with rates decreasing to 20 per million for ages 8 to 10 years." - NCI 2002 [1]
-
NCI - for Health Professionals
Important: review links at the bottom of the NCI site for studies related to treatment.
-
About Adult Acute Lymphoblastic Leukemia Cancer.gov
-
BiTE Antibody Blinatumomab Receives European Orphan Drug Designation for Treatment of Acute Lymphoblastic Leukemia (ALL) prnewswire.com | About BiTE
|
Epstein-Barr Virus Associated Lymphoma
|
Epstein-Barr Associated Lymphoma
|
Current understanding of the role of Epstein-Barr virus (EBV) in lymphomagenesis and therapeutic approaches to EBV-associated lymphomas http://bit.ly/bx6s44 (2008)
Jeffrey I. Cohen, 1 Catherine M. Bollard,2 Rajiv Khanna,3 and Stefania Pittaluga4 1 Catherine M. Bollard,2 Rajiv Khanna,3 and Stefania Pittaluga4
“The great majority of people carry latent EBV all their lives without any symptoms, but in certain circumstances latent EBV infection is associated with EBV-positive malignancies, which include
Burkitt’s lymphoma,
B-cell lymphoproliferative diseases,
Hodgkin’s lymphoma (HL), and
T-cell lymphomas.
Following primary EBV infection, individuals remain lifelong carriers of the virus. In vivo, B lymphocytes infected with the EBV are initially controlled by natural killer (NK) cells and cytotoxic T lymphocytes (CTL) [Hislop 2007]. However, the initial CTL response does not remove all the EBV-infected B cells and a pool of memory B cells latently infected with EBV becomes established.
...
EBV-positive lymphomas can be divided into those occurring in immunodeficient individuals, which are true virally driven lymphomas, such as PTLD and HIV-associated immunoblastic lymphoma, and those occurring in immunocompetent individuals.
The latter group includes endemic and sporadic Burkitt’s lymphoma, and some T-and NK-cell malignancies. In these malignancies occurring in immunocompetent individuals, EBV is a cofactor rather than the driving influence [Khanna 2005]."
Related Reports
* Comprehensive profiling of functional Epstein-Barr virus miRNA expression in human cell lines, full text - Europe PMC http://bit.ly/2bg52qv
* 2016 - Full Report: Phase I Trial of 4-1BB-based Adoptive T-Cell Therapy for Epstein-Barr Virus positive tumors http://bit.ly/28OZwoX
* LMP1/2-Specific Cytotoxic T Lymphocytes for EBV-Associated Lymphoma -
ClinicalTrials.gov http://1.usa.gov/1bj4FGm
Clinical report, PubMed:
Clinical Trials and Observations: Complete responses of relapsed lymphoma following genetic modification of tumor-antigen presenting cells and T-lymphocyte transfer http://1.usa.gov/1kvF13T
We have now used gene transfer into antigen-presenting cells (APCs) to augment the expression and immunogenicity of LMP2. These modified APCs increased the frequency of LMP2-specific CTLs by up to 100-fold compared with unmodified LCL-APCs. The LMP2-specific population expanded and persisted in vivo without adverse effects. Nine of 10 patients treated in remission of high-risk disease remain in remission, and 5 of 6 patients with active relapsed disease had a tumor response, which was complete in 4 and sustained for more than 9 months. It is therefore possible to generate immune responses to weak tumor antigens by ex vivo genetic modification of APCs and the CTLs so produced can have substantial antitumor activity.
Technical background article:
* Manufacture of GMP-grade Cytotoxic T Lymphocytes specific for LMP1 and LMP2 for Patients with EBV-associated Lymphoma http://1.usa.gov/1gm11ZK
|
Burkitt's
|
Burkitt's
|
We have moved this topic to a new page.
See Burkitt's lymphomas
|
Grey Zone lymphomas
|
|
TOPIC SEARCH: Euro-Med
|
Grey Zone lymphomas
|
"Mediastinal gray-zone lymphoma lies intermediate between nodular-sclerosis classic Hodgkin’s lymphoma and primary mediastinal B-cell lymphoma (a subtype of diffuse large B-cell lymphoma) [2]
-
Pitfalls in diagnostic hematopathology
-
2017
PD-1 Blockade in Mediastinal Gray-Zone Lymphoma — NEJM http://bit.ly/2sIKvjc
"The high frequency of 9p24.1 copy-number alterations across mediastinal lymphomas suggests a disease-specific, genetically determined dependence on PD-1 for survival. These cases provide early evidence for using PD-1 inhibition in relapsed or refractory mediastinal gray-zone lymphoma, which warrants further testing."
|
Nasopharynx lymphomas
|
|
TOPIC SEARCH: Euro-Med
|
Nasopharynx lymphomas
cell of origin varies
|
Nasopharyngeal lymphomas are rare. The underlying histology (cell of origin) varies. It can be DLBCL, Hodgkin's, t-cell, follicular, or marginal zone.
We feel it's prudent to arrange for a second evaluation of the biopsy sample for this diagnosis and to seek an expert second opinion on the approach to treatment and management from a major center.
.gif) |
Primary Nasopharyngeal non-Hodgkin lymphomas: a retrospective review of 26 Moroccan patients | BMC Ear, Nose and Throat Disorders | Full Text http://bit.ly/2riCsMt
|
|
Diffuse Large B-Cell Lymphoma of the Nasopharynx Presenting With Cluster-Like Headache.
|
|
Nasopharyngeal Hodgkin Lymphoma ascopubs.org
|
|
Lymphoid granulomatosi
|
"Lymphomatoid granulomatosis is a rare angiocentric and angiodestructive disease, which commonly involves the lungs but also the brain, kidneys, liver and skin." [3] which is frequently associated with Epstein-Barr virus infection. [4]
"The pathogenesis of LYG is unknown; however, recent studies have provided overwhelming evidence that LYG is a distinctive type of malignant lymphoma associated with immunosuppression." e-medicine
-
About e-medicine
-
Successful treatment of mediastinal lymphomatoid granulomatosis with rituximab monotherapy. Eur J Haematol. 2005 Mar;74(3):263-6. PMID: 15693798 | Related articles
-
Fatal haemoptysis in a case of lymphomatoid granulomatosis treated with rituximab.
Eur Respir J. 2006 Mar;27(3):644-6. PMID: 16507866
-
[Efficacy of rituximab in lymphomatoid granulomatosis] Rev Mal Respir. 2004 Dec;21(6 Pt 1):1157-61. French. PMID: 15767962 | Related articles
-
Pulmonary lymphomatoid granulomatosis. Evidence for a proliferation of Epstein-Barr virus infected B-lymphocytes with a prominent T-cell component and vasculitis.
Am J Surg Pathol. 1994 Aug;18(8):753-64. PMID: 8037289
|
Lymphoid granulomatosis (LYG)
|
|
TOPIC SEARCH: PubMed
|
Lymphoid granulomatosi
|
"Lymphomatoid granulomatosis is a rare angiocentric and angiodestructive disease, which commonly involves the lungs but also the brain, kidneys, liver and skin." [3] which is frequently associated with Epstein-Barr virus infection. [4]
"The pathogenesis of LYG is unknown; however, recent studies have provided overwhelming evidence that LYG is a distinctive type of malignant lymphoma associated with immunosuppression." e-medicine
-
About e-medicine
-
Successful treatment of mediastinal lymphomatoid granulomatosis with rituximab monotherapy. Eur J Haematol. 2005 Mar;74(3):263-6. PMID: 15693798 | Related articles
-
Fatal haemoptysis in a case of lymphomatoid granulomatosis treated with rituximab.
Eur Respir J. 2006 Mar;27(3):644-6. PMID: 16507866
-
[Efficacy of rituximab in lymphomatoid granulomatosis] Rev Mal Respir. 2004 Dec;21(6 Pt 1):1157-61. French. PMID: 15767962 | Related articles
-
Pulmonary lymphomatoid granulomatosis. Evidence for a proliferation of Epstein-Barr virus infected B-lymphocytes with a prominent T-cell component and vasculitis.
Am J Surg Pathol. 1994 Aug;18(8):753-64. PMID: 8037289
|
Splenic Lymphoma with Villous Lymphocytes
|
|
TOPIC SEARCH: PubMed
|
Splenic Lymphoma with Villous Lymphocytes
B-cell stage: mature, before antigen exposure
Associated with
hepatitis C virus
Often misdiagnosed as CLL
|
"Splenic lymphoma with villous lymphocytes (SLVL) is a recently recognized entity among chronic B lymphoproliferative disorders. It has a distinct clinical, morphological and immunophenotypic pattern and was previously described under a variety of designations. SLVL can be misdiagnosed as chronic lymphocytic leukemia (CLL), prolymphocytic leukemia (PLL), or hairy cell leukemia (HCL)." kfshrc.edu.sa
Also see: Marginal Zone - Splenic
|
About infobiogen.fr
|
|
Splenic lymphoma in presence of HCV may respond to interferon alpha Reuters Health Jul_10_02 (link repaired May 2004) And see mediscover.net
|
|
Dramatic efficacy of Fludarabine in the treatment of an aggressive case of splenic lymphoma with villous lymphocytes. Eur J Haematol. 2002 Aug;69(2):112-4. PMID: 12366716 PubMed
|
|
Regression of splenic lymphoma with villous lymphocytes after treatment of hepatitis C virus infection. N Engl J Med. 2002 Jul 11;347(2):89-94. PMID: 12110736 PubMed
|
|
Cyclin D3 is a target gene of t(6;14)(p21.1;q32.3) of mature B-cell malignancies. Blood. 2001 Nov 1;98(9):2837-44. abstract | related abstracts
|
|
Waldeyer's ring lymphomas
|
|
TOPIC SEARCH: ASCO | Medscape | PubMed
|
Waldeyer's ring lymphomas
|
"It is debated whether non-Hodgkin's lymphomas originating in Waldeyer's ring (WR NHL) behave as NHL originating in lymph nodes or share common features with extranodal lymphomas originating in mucosa associated lymphatic tissue (MALT).
We analyzed data from a population based NHL registry on patterns of dissemination at diagnosis, response to treatment, patterns of failure and survival of 77 primary Waldeyer's ring Non-Hodgkin's lymphomas (WR NHL) patents. Data of completely staged patients with diffuse large cell lymphomas (DLCL) originating in WR (n=44) were compared with those of patients retrieved from the same registry with DLCL originating in lymph nodes or stomach (the latter as prototype of a lymphoma originating in MALT).
Primary WR NHL had favorable risk scores according to the International Prognostic Index (IPI), and responded well to therapy: a complete response (CR) rate of 74% was observed.
Disease free survival (DFS) and overall survival (OS) were poor, however (47% and 31% at 10 years, respectively). The comparison of DLCL originating in WR, lymph nodes and stomach revealed that WR and gastric NHL patients shared a restricted pattern of dissemination at diagnosis, in contrast to patients with DLCL originating in lymph nodes." 1
-
Waldeyer's ring lymphomas: a clinical study from the Comprehensive Cancer Center West population based NHL registry. Leuk Lymphoma. 2001 Sep-Oct;42(5):1005-13.
PMID: 11697617
-
Waldeyer's ring lymphomas: the prognostic factors and the treatment outcome Year: 2002 Abstract No: 1138
|
Post Transplant Lymphoproliferative Disorder (PTLD)
|
|
TOPIC SEARCH: ASCO | ClinicalTrials.gov | Medscape | PubMed
|
Post Transplant Lymphoproliferative Disorder (PTLD)
|
"Post-transplant lymphoproliferative disorders (PTLD) are a diverse group of abnormal lymphoid [a type of white blood cell] growths that include both hyperplasias [An abnormal increase in the number of cells in an organ or tissue]
They have been divided into several general pathologic categories that have prognostic [outcome] significance. These include early or hyperplastic PTLD, polymorphic PTLD, and lymphomatous or monomorphic PTLD.
The majority of PTLDs are of B-cell origin and contain Epstein-Barr virus (EBV). However, PTLDs of T- or NK-cell origin have been described, and late-arising EBV-negative lymphoid tumors are becoming more frequently reported in this population." 3
-
Discovery of mechanism that may explain post-transplant lymphoproliferative disorder newsmedicinenet
-
Post-transplant lymphoproliferative disorder is the most common malignancy, with the exception of skin cancer, after solid organ transplantation in adults.
The incidence varies according to the transplanted organ and is often associated with Epstein-Barr virus. Prognosis is variable, due in part to the heterogeneity of the disease, which ranges from reactive plasmacytic hyperplasia to aggressive monoclonal disease. oncologist
-
The diverse pathology of post-transplant lymphoproliferative disorders: the importance of a standardized approach. Transpl Infect Dis. 2001 Jun;3(2):88-96. Review.
PMID: 11395974
|
Other uncommon Lymphomas or pseudo-tumors
|
Other lymphomas
|
|
Follicular Hyperplasia, Follicular Lysis, and Progressive Transformation of Germinal Centers A Sequential Spectrum of Morphologic Evolution in Lymphoid Hyperplasia
http://ajcp.ascpjournals.org/content/120/3/322.full.pdf
|
|
Primary cardiac diffuse large B cell lymphoma presenting with superior vena cava syndrome http://www.ncbi.nlm.nih.gov/pubmed/19536397
"Primary cardiac lymphomas are rare extranodal lymphomas that should be distinguished from secondary cardiac involvement by disseminated non-Hodgkin's lymphoma. Cardiac lymphomas often mimic other cardiac neoplasms, including myxomas and angiosarcomas, and often require multimodality cardiac imaging, in combination with endomyocardial biopsy, excisional biopsy or pericardial fluid cytology, to establish a definitive diagnosis."
|
|
Lmphoplasmacytic lymphoma, see WM
|
|
Thyroid Lymphoma emedicine
|
|
|
|
Castleman's disease is associated with lymphoma:
"Castleman's disease (CD) is a rare atypical lymphoproliferative disorder whose morphology, soon after the original presentation of Castleman et al., has been definitely subdivided in a hyaline vascular (HV) and plasma cell (PC) histopathological pattern, with intermediate variants. The former occurs much more frequently than the latter" 3
-
Mayo Clinic background on Castleman's disease mayoclinic.com
-
NCBI - Three patients with both Hodgkin's lymphoma and Castleman's disease: Clinicopathologic correlations and lack of association with HHV-8 ncbi.nlm.nih.gov
-
NCBI - Castleman's disease. ncbi.nlm.nih.gov
|
|
{kind=link}