|
Types of Lymphoma > Mantle Cell Lymphoma (MCL)
Last update: 05/28/2019
|
|
TOPICS:
Overview | Workup | Treatments | Clinical Trials | Research News
 TOPIC SEARCH: PubMed: Diagnosis | Review | Therapies | Prognosis TOPIC SEARCH: PubMed: Diagnosis | Review | Therapies | Prognosis
|
About Lymphomas
Overview of genes and cancer
Lymphoma Overview
|
Mantle Cell Lymphoma
Mantle Cell lymphoma (MCL) is a cancer of b-cells (lymphocytes) - a type of blood cell that protects against infection as part of the immune system.
Most lymphoma develop from an acquired (not inherited) injury to the DNA in the genes of a single cell - the cell of origin. ... The defects are passed on with each cell division, giving the defective lymphocytes a growth and survival advantages over normal cells. So when a lymphoma develops cell division is not balanced by cell death. The abnormal cells eventually accumulate to form tumors most commonly in the lymph glands.
The median age at diagnosis for MCL is between 60-70 years and most affected by this condition are men (75-80%). It's an uncommon type of lymphoma - about 7% of all non-Hodgkins lymphoma.
MCL is almost always widespread (systemic) when diagnosed -- showing as stage III/IV disease with "extra nodal involvement" - meaning that tumors may also form outside of the Lymphatic System.
As of this writing (2013), the regular way to treat MCL has been focused on aggressive first treatment for younger patients - with an option for transplant. Aggressive treatment is often effective, increasingly of late, however the disease-free remissions do not always last and the side effects of these treatment can be significant. Effective therapies for the elderly or relapsed patient have been limited. Responses to less aggressive therapies are good, but short-lived, and options at relapse, until recently have been limited.
It is challenging to do well-powered studies for MCL because of differences in the approach by age and that MCL is uncommon - and differences in the philosophy - by center - on how to treat MCL with the same risk factors.
Technical - pathology:
Characteristic cell surface protein expression demonstrates monoclonal (all from same cell of origin) B cells that co-express CD5, a normal T cell marker, but not CD23, differentiating MCL from the more common CD5+ B cell disorder chronic lymphocytic leukemia (CLL).
References
Overview of MCL - 2012
update on diagnosis, risk-stratification, and clinical management
Best Pract Res Clin Haematol, 2013:
Novel Agents in Mantle Cell Lymphoma http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3374151/
Patient Perspective: comments on research focus for MCL - draft
Incidence
Mantle Cell Lymphoma represents 4% to 8% of non-Hodgkin’s lymphomas. It primarily affects older individuals; males more than females by a ratio of about 4 to 1. The median age at diagnosis is approximately 58 years of age.
The incidence of MCL increased from 1992 to 2004, and was significantly higher in men, in Caucasians, and patients aged > or =50 years. Most patients were diagnosed with late-stage MCL, and there also were considerable geographic variations observed in incidence rate.
Table 1. Incidence of Mantle Cell Lymphoma by Age, Sex, Race, Tumor Stage, and Geographic Region (1992-2004)
| |
Age-adjusted Incidence Rate per 100,000 (95% CI - Confidence Interval)* |
Relative Risk (95% CI) |
|
|
| Age, y |
|
|
| <50 |
0.07 (0.06-0.08) |
1.00 |
| 50-59 |
0.83 (0.76-0.92) |
11.72 (10.00-13.76) |
| 60-69 |
1.96 (1.81-2.12) |
27.55 (23.77-32.01) |
| 70-79 |
2.97 (2.76-3.19) |
41.70 (36.08-48.34) |
| ≥80 |
2.78 (2.51-3.07) |
39.10 (33.29-45.99) |
Cancer. 2008 Aug 15;113(4):791-8. doi: 10.1002/cncr.23608.
Incidence trends of mantle cell lymphoma in the United States between 1992 and 2004.
Zhou Y, Wang H, Fang W, Romaguer JE, Zhang Y, Delasalle KB, Kwak L, Yi Q, Du XL, Wang M.
http://onlinelibrary.wiley.com/doi/10.1002/cncr.23608/full
Diagnosis
To make an accurate diagnosis of lymphoma, a biopsy must be performed by the surgical removal (resection) of a lymph node. A fine needle aspiration may be performed if a lymph node is not accessible, but this is not considered a definitive way to determine the diagnosis.
A series of tests will then be performed to determine the characteristics of the cells. If a malignancy is determine, these characteristics will allow your doctors to determine the appropriate treatments to use when needed.
Workup (adapted from NCCN Guidelines 2010)
.gif) |
Staging tests:
|
CT of Chest/abdominal/pelvic with contrast of diagnostic quality
|
|
Bone marrow biopsy + aspirate to document clinical stage I_II disease
|
|
Useful in select cases:
|
Endoscopy/colonoscopy
|
|
Lumbar puncture (for blastic variant or CNS symptoms)
|
|
PET-CT scan
|
|
CT of neck
|
|
|
|
Physical exam:
|
Attention to node-bearing areas, including Waldeyer's ring
|
|
Examine size of liver and spleen
|
|
Performance status
|
|
B symptoms
|
|
|
Labs and tests:
|
CBC, differential, platelets,
|
|
LDH
|
|
Comprehensive metabolic panel
|
|
Hepatitis B testing
|
|
Useful in select cases:
|
Hepatitis C test
|
|
Uric acid
|
|
Beta-2-microglobulin
|
|
|
|
Treatment, age and gender specific:
|
MUGA scan / echocardiogram"
(prior to anthracycline-based therapy)
|
|
Discuss fertility issues
|
|
Pregnancy testing in women of child-bearing age if chemo is planned
|
|
Workup
See for details e-medicine
Common symptoms
|
fatigue (anemia)
|
|
loss of appetite
|
|
feeling of fullness or discomfort due to enlarged liver or spleen
|
|
enlarged lymph nodes - painless swelling in the neck, armpit or groin - often in more than one group
|
Other symptoms may include night sweats, unexplained high temperatures and weight loss. These are known as B symptoms.
Resources
|
About Emedicine | LLS
|
|
ASCO Ed: Current Approaches (2017) to Mantle Cell Lymphoma: Diagnosis, Prognosis, and Therapies http://bit.ly/2qOdP61
|
|
Mantle Cell Lymphoma: Background for physicians
Medscape.com (free login req.)
Mantle cell lymphoma (MCL), which represents approximately 6% of non-Hodgkin's lymphoma (NHL) cases, remains the most challenging lymphoma to treat. As a result, this is one of the most active areas of investigation in lymphoma, in terms of translational research as well as in the development of novel approaches, some of which will be highlighted in this review.
|
|
Non-Hodgkins Lymphomas - Clinical Practice Guidelines in Oncology
nccn.org professionals pdf (one-time free registration and login required)
|
|
Genetics Cancer Genetics Web
|
|
Mantle Cell Information Websites mclresource.com/MCLAid
|
|
CD5- Mantle Cell Lymphoma: from American Journal of Clinical Pathology - Medscape (free login req.)
"Mantle cell lymphoma (MCL) typically expresses B-cell antigens and CD5 and overexpresses bcl-1 protein. However, unusual cases of bcl-1+ and CD5- MCL have been observed, posing a practical challenge for correct diagnosis and management."
|
|
Mantle Cell Lymphoma: Background Medscape.com (free login req.)
Mantle cell lymphoma (MCL), which represents approximately 6% of non-Hodgkin's lymphoma (NHL) cases, remains the most challenging lymphoma to treat. As a result, this is one of the most active areas of investigation in lymphoma, in terms of translational research as well as in the development of novel approaches, some of which will be highlighted in this review.
|
Variants:
|
Limited-stage mantle-cell lymphoma annonc.oxfordjournals.org
H. A. Leitch1, R. D. Gascoyne2, M. Chhanabhai2, N. J. Voss3, R. Klasa1 and J. M. Connors
|
|
Indolent MCL with nodal involvement and mutated immunoglobulin heavy chain genes humanpathol.com
We present a case of an indolent MCL that was documented with cyclin D1 expression in a lymph node biopsy performed more than 12 years ago. The patient has peripheral blood involvement with a lymphocyte count in the reference range, variable thrombocytopenia, and minimal adenopathy but is otherwise well, never having received any antineoplastic therapy.
|
|
Treatments
|
Treatment Articles
 TOPIC SEARCH to keep current! TOPIC SEARCH to keep current!
PubMed: Review | Therapies | Stem Cell Transplant
Google Scholar: MCL and Maintenance
Also see Protocols for Refractory Disease PAL
Clinical Trials for MCL PAL
Reasons to be encouraged: Our sense is that progress against MCL is advancing rapidly of late for many reasons. What is most appropriate as therapy is highly individualized in MCL ... so do consult experts directly. We also suggest that MCL survivors inquire specifically about clinical trials.
Nov 2017: FDA Approves Acalabrutinib (btk inhibitor) for Mantle Cell Lymphoma http://bit.ly/2imGOM3
At a median follow-up of 15.2 months, the ORR by independent review committee was 80% (95% CI, 72%-87%), which was comprised evenly of CR and PR rates of 40%. The median duration of response was not yet reached at the time of analysis, with responses ongoing at 20+ months. The median time to best response was 1.9 months.
Overview on Treatment of MCL:
|
|
|
Current and Novel Therapies for Mantle Cell Lymphoma cme.medscape.com/
"The purine nucleoside analogues (PNAs) also have activity as single agents and in combination with rituximab; they are ideal regimens for older patients and patients who are not eligible for SCT. Recent studies in patients with relapsed MCL have shown substantial antitumor activity of bortezomib, the mTOR inhibitors temsirolimus and everolimus, the immunomodulatory drugs thalidomide and lenalidomide, and Bendamustine. Studies integrating these novel agents earlier in the disease course or in combination with each other will, we hope, produce more durable responses with less toxicity."
|
Stem cell rescue (transplant):
|
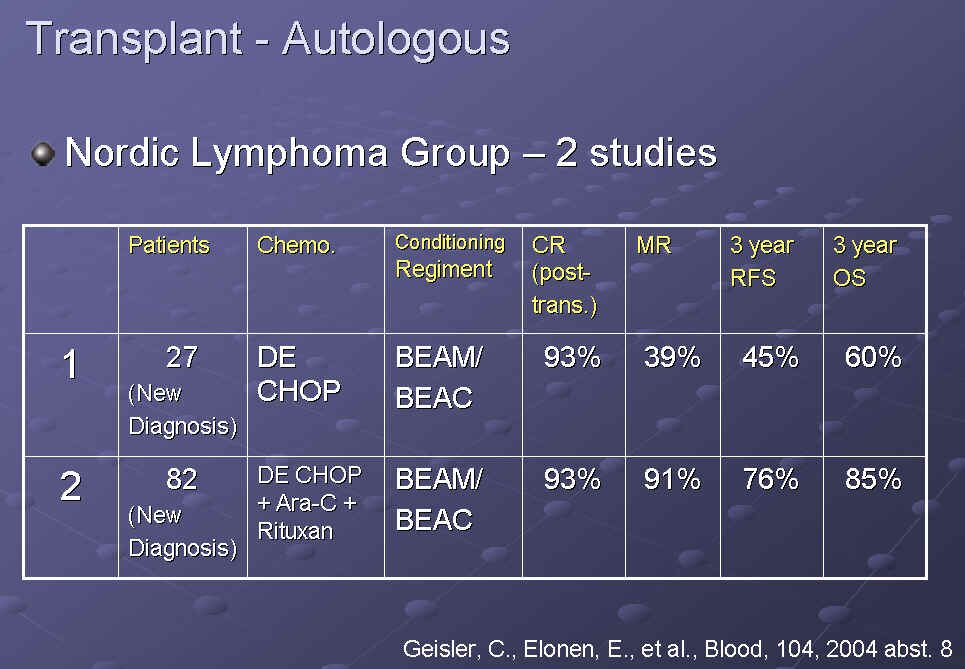
ARA-C incorporation into SCT (Nordic group) Protocol
 click to enlarge click to enlarge
|
|
The Nordic group's conclusion: "The addition of high dose ARA-C and Rituxan increased event-free, progression-free, and overall survival; that the molecular remission rate and the duration of remission was better; and interestingly - they collected stem cells after the therapy - the proportion of PCR-negative stem cell product was less.
... that the 5-year event-free survival plateau of 63% suggests this treatment may be - and the editorial quotes here are my own, they are not in their presentation- Curative. But their suggestion is that progression-free survival is higher than anything we have seen before, so these are interesting data." Dr. Gordon (NCCN updates)
|
|
~ Long-term progression-free survival of MCL following intensive front-line immunochemotherapy with in vivo-purged stem cell rescue:
A non-randomized phase-II multicenter study by the Nordic Lymphoma Group. Blood. 2008 Jul 14.
full text bloodjournal.hematologylibrary.org
n = 160 consecutive, untreated patients younger than 66 years
|
|
MCL Can Be Cured by Intensive Immunochemotherapy with In-Vivo Purged Stem-Cell Support; Final Report of the Nordic Lymphoma Group MCL2 Study ASH abstracts2view.com
Conclusion: The demonstration of long-term event-free survival in a large, consecutive prospective series now for the first time indicates that intensive immunochemotherapy including AraC and Rituximab with in-vivo purged stem-cell support may cure mantle cell lymphoma.
|
|
The Role of Autologous Transplantation in the Management of Mantle Cell Lymphoma: A Study From the EBMT , E. Vandenberghe, et al. PDF - mmserver.cjp.com
|
|
Review of :"Long-term remission in mantle-cell lymphoma following high-dose sequential chemotherapy and in vivo rituxan-purged stem cell autografting (R-HDS regimen)" Blood Docguide.com
|
|
The Role of Autologous Transplantation in the Management of Mantle Cell Lymphoma: PDF
|
|
" Mini " Transplants Effective in Recurrent Mantle Cell cancerconsultants.com
|
|
Tandem Transplants:
Patients with mantle-cell lymphoma relapsing after autologous stem cell transplantation may be rescued by allogeneic transplantation. Bone Marrow Transplant. 2000 Sep;26(6):677-9. PMID: 11035375 PubMed
|
|
Hyper CVAD Followed by SCT for MCL PubMed
|
|
Radioimmunotherapy:
|
Radioimmunotherapy Consolidation in Mantle Cell Lymphoma http://bit.ly/9kt6WK PDF http://bit.ly/c7HIxm
Wojciech Jurczak, European Oncological Disease - Published: October 2008
A thorough description of the rationale for consolidation with RIT for MCL – but also informative for other lymphomas.
|
|
High-Dose Iodine-131-Labeled Rituxan and Autologous Stem Cell Support Produces Long Lasting Effects in Patients with Mantle Cell Lymphoma Failing Conventional Autologous Transplants cancerconsultants.com
Also see full text: bloodjournal.hematologylibrary.org
|
|
Zevalin in Mantle Cell Lymphoma touchbriefings.com pdf
Conclusion: Radiotherapy is an active treatment modality in MCL. Ibritumomab radioimmunotherapy (Zevalin) is an interesting alternative to other consolidation methods. In younger patients subjected to intensive chemotherapy followed by autologous transplant, it may be an element of a transplant conditioning regimen (i.e. Z-BEAM). In elderly patients, the role of zevalin consolidation should be further investigated in a phase III trial.
|
|
Studies presented at ASH explore activity of the Bexxar® therapeutic regimen in difficult-to-treat lymphomas www.icaa.eu
|
|
|
Targeted / Immune-based Therapy:
|
Lenalidomide (Revlimid) Oral Monotherapy in Patients with Mantle
Cell Lymphoma Previously Treated with Bortezomib (Velcade) http://bit.ly/VandR
|
|
Revlimid® Active for Treating Mantle Cell Lymphoma cancerconsultants.com
n = 15 patients with mantle cell lymphoma who had failed prior therapy, including stem cell transplantation in five.
The overall response rate was 53% with 20% (n=3) having a complete response. The median duration of response was 14 months, and the median progression-free survival was 5.6 months. Four of the five patients who had failed stem cell transplantation responded.
|
|
Temsirolimus (mTOR inhibitor) Promising for Treatment of MCL and other cancers cancerconsultants.com
|
|
Managing and avoiding bortezomib (Velcade) toxicity
Jeffrey Menashe, MD | Northwest Cancer Specialists, Portland, OR
communityoncology.net pdf
|
|
Response to thalidomide in chemotherapy-resistant mantle cell lymphoma: a case report. Br J Haematol. 2002 Oct;119(1):128-30. PMID: 12358916 PubMed
|
|
Phase II Trial of Single-Agent Temsirolimus (CCI-779) for Relapsed Mantle Cell Lymphoma. J Clin Oncol. 2005 Jun 27 PMID: 15983389
|
|
A low toxicity maintenance regime, using eicosapentaenoic acid and readily available drugs, for mantle cell lymphoma and other malignancies with excess cyclin D1 levels. Med Hypotheses. 2003 May;60(5):615-23. PMID: 12710892 PubMed
|
|
Velcade: Inhibition of the proteasome induces cell cycle arrest and apoptosis in mantle cell lymphoma cells. Br J Haematol. 2003 Jul;122(2):260-8. PMID: 12846895 PubMed
|
|
|
Combination therapy:
|
Phase II multicenter study of bendamustine plus Rituxan in patients with relapsed indolent B-cell and mantle cell NHL.
J Clin Oncol. 2008 Sep 20;26(27):4473-9. Epub 2008 Jul 14. PMID: 18626004
(n = 66 patients with relapsed, indolent B-cell or mantle cell lymphoma (without documented resistance to prior rituximab)
Overall response rate was 92% (41% complete response, 14% unconfirmed complete response, and 38% partial response). Median duration of response was 21 months (95% CI, 18 to 24 months). Median progression-free survival time was 23 months (95% CI, 20 to 26 months). Outcomes were similar for patients with indolent or mantle cell histologies.
|
|
|
Fludarabine-based chemotherapy in untreated mantle cell lymphomas:
an encouraging experience in 29 patients PIER LUIGI ZINZANI et al. - Haematologica 1999; 84:1002-1006 PDF
|
Other Treatment-related items:
|
Standard Therapy for Mantle Cell Lymphoma? http://bit.ly/htWQpf
|
|
Ki-67 as a prognostic marker in MCL—consensus guidelines of the pathology panel of the European MCL Network ncbi.nlm.nih.gov
|
|
RQ-PCR Positivity Predicts Relapse of Mantle Cell Lymphoma
after Autologous Stem Cell Transplant cancerconsultants.com
The researchers concluded that the presence of MRD (minimal residual disease) following an AutoSCT in patients with MCL is highly predictive of outcomes in this group of patients. The authors suggest testing for MRD in this group of patients; those with MRD may benefit from additional or more aggressive therapies.
|
|
Mantle Cell treatment effective BBCNews
|
|
Mantle cell lymphoma involving skin: cutaneous lesions may be the first manifestation of disease and tumors often have blastoid cytologic features. Am J Surg Pathol. 2002 Oct;26(10):1312-8. PMID: 12360046 PubMed
|
|
Clinical Trials
|
ClinicalTrials.gov
|
Study of interest:
Comparing Bendamustine and Rituximab (BR) Alone to BR given with Acalabrutinib (btk-inhibitor) in Patients over 65 years of age with Previously Untreated Mantle Cell Lymphoma - ClinicalTrials.gov http://bit.ly/2OBnYUw
See also the Sponsor's IRB-approved background: pdf
|
|
All studies
|
|
Newly Diagnosed or untreated
|
|
Recurrent
|
Excluding stem cell transplant (by request)
|
|
|
|
|
|
|
|
|
Research News
|
In the News and Research News
|
FDA Approves Acalabrutinib (btk inhibitor) for Mantle Cell Lymphoma http://bit.ly/2imGOM3
At a median follow-up of 15.2 months, the ORR by independent review committee was 80% (95% CI, 72%-87%), which was comprised evenly of CR and PR rates of 40%. The median duration of response was not yet reached at the time of analysis, with responses ongoing at 20+ months. The median time to best response was 1.9 months.
Of the 124 patients in the phase II trial, 80 were ≥65 years of age and 32 were ≥75 years. Overall, there were no meaningful efficacy differences observed between those ≥65 years of age and those younger. Additionally, the safety profile was similar between the two age groups, according to the FDA.
The most common adverse events (AEs) of any grade were anemia (46%), thrombocytopenia (44%), headache (39%), neutropenia (36%), diarrhea (31%), fatigue (28%), myalgia (21%), and bruising (21%). The most common grade ≥3 AEs were neutropenia (15%), thrombocytopenia (12%), anemia (10%), and diarrhea (3.2%).
Serious AEs associated with acalabrutinib included hemorrhage, infections, and atrial fibrillation. In a database of 612 patients treated with acalabrutinib monotherapy across clinical trials, 18% of patients experienced grade ≥3 infections, most frequently pneumonia. In this safety group, atrial fibrillation and atrial flutter of any grade occurred in 3% of patients, with 1% having a grade 3 event. Overall, bleeding, bruising, or petechiae events of any grade occurred in approximately 50% of patients, with grade ≥3 events seen in 2% of patients.
The median duration of treatment with acalabrutinib was 16.6 months (range, 0.1-26.6), with 73.4% of patients receiving the medication for ≥6 months and 59.7% of patients on treatment for ≥1 year. Overall, dose reductions due to AEs were required for 1.6% of patients and dose discontinuations were required for 6.5%.
|
|
Acalabrutinib received an FDA breakthrough designation for the treatment of Mantle Cell Lymphoma.
This designation is given when "preliminary clinical evidence indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development."
Here’s the (no-longer recruiting) study that’s the likely basis for the breakthrough designation:
https://clinicaltrials.gov/show/NCT02213926
Acalabrutinib (ACP-196): a selective second-generation BTK inhibitor | Journal of Hematology & Oncology | Full Text http://bit.ly/2vojqWv
"Acalabrutinib (ACP-196) is a novel irreversible second-generation BTK inhibitor that was shown to be more potent and selective than ibrutinib. This review summarized the preclinical research and clinical data of acalabrutinib."
Comment: Acalabrutinib is in the same class as Ibrutinib (similar target, also an oral drug). Ibrutinib is already approved for use in MCL. So we might safely assume that the efficacy and/or safety appears to be substantially better for Acalabrutinib. However, I could not find an published reports on outcomes in the trial above - nor a statement by FDA on the basis for the decision. In any case, it's very big and good news.
Fact Sheet: FDA Breakthrough Therapies http://bit.ly/2uYNN3y
|
|
ASH paper: The EBMT Lymphoma Working Party-European Mantle Cell Lymphoma Network
Consensus On Role Of Transplant: http://bit.ly/IyzAkv
ASH Paper: The Ribvd Regimen- High CR Rate In Elderly Patients With Untx MC
Lymphoma. Preliminary Results http://bit.ly/1ct61fb
ASH Paper: The Single-Agent Bcl-2 Inhibitor ABT-199 (GDC-0199) In Patients With
Relapsed/Refractory http://bit.ly/1b1rOM4
ASH Paper: Exploratory Ki-67 Results - Study Of Lenalidomide In Mantle Cell
Lymphoma Relapsed Or Refractory To Bortez http://bit.ly/ISXaZc
|
|
J Clin Onc 2013:
Autologous or Reduced-Intensity Conditioning Allogeneic Hematopoietic Cell Transplantation for Chemotherapy-Sensitive Mantle-Cell Lymphoma: Analysis of Transplantation Timing and Modality. http://1.usa.gov/19kwbCr
|
|
ASH Papers:
Len, Benda, and Rituxan As 1st-Line Therapy For Patients >65 Years w Mantle Cell Lymphoma: Prelim Results http://bit.ly/1d2Hls1
Presently, 29 patients are evaluable for response after 6 cycles LBR. ORR is 28/29 (97%), CR+CRu 23 (79%). 17 out of 28 evaluable patients (61%) were MRD-negative after 6 cycles. After a median follow-up of 18 months, the median PFS has not been reached, and the estimated PFS at 2 years is 74%.
ASH Paper: The Ribvd Regimen- High CR Rate In Elderly Patients With Untx MC Lymphoma. Preliminary Results http://bit.ly/1ct61fb
ASH paper: The EBMT Lymphoma Working Party-European Mantle Cell Lymphoma Network Consensus On Role Of Transplant: http://bit.ly/IyzAkv
ASH Paper: Exploratory Ki-67 Results - Study Of Lenalidomide In Mantle Cell Lymphoma Relapsed Or Refractory To Bortez http://bit.ly/ISXaZc
Ki-67 shows proliferation rate of cells.
ASH Paper: Radioimmunotherapy In Relapsed/Refractory Mantle Cell Lymphoma Patients: Final Results Of Network Trial http://bit.ly/1eYt4yf
|
ASH papers - Mixed types, including MCL:
The Single-Agent Bcl-2 Inhibitor ABT-199 (GDC-0199) In Patients With Relapsed/Refractory http://bit.ly/1b1rOM4
Encouraging with 100% ORR for MCL
A Phase I Study Of Myeloablative Radioimmunotherapy Using Iodine-131 Anti-CD45 Antibody Followed By Autologous Stem Cell Transplantation For High-Risk B-Cell and T-Cell Non-Hodgkin Lymphoma and Hodgkin Lymphoma http://bit.ly/1jprN3H
Second Allogeneic Stem Cell Transplantation (AlloSCT) In Patients With Relapsed Lymphoma After First Allosct. A Retrospective Study Of The EBMT Lymphoma Working Party http://bit.ly/J137nE
|
|
Am J Hematology 2013:
Mantle cell lymphoma: 2013 Update on diagnosis, risk-stratification, and clinical management. http://1.usa.gov/19awnOH
For selected indolent, low MIPI MCL patients, initial observation may be appropriate therapy. For younger patients with intermediate or high risk MIPI MCL, aggressive therapy with a cytarabine containing regimen ± autologous stem cell transplantation should be considered. For older MCL patients with intermediate or high risk MIPI, combination chemotherapy with R-CHOP, R-Bendamustine, or a clinical trial should be considered. At the time of relapse ...
|
|
April 2013:
Pharmacyclics Completes Enrollment of Phase III Ibrutinib CLL Study and Phase II Ibrutinib MCL Study ascopost.com
|
|
Medpage today:
Combo Tx Gets Perfect Score in Mantle Cell Lymphoma http://bit.ly/12OInDA
|
|
Visco C. J Clin Oncol.2013
R-BAC shows promise in mantle cell lymphoma http://bit.ly/16pBrj2
|
|
|
|
Video - Patient Power: Dr. Peter Martin on Kinase Inhibitors Offer New Hope for Mantle Cell Lymphoma http://bit.ly/KwigwH
|
|
MCL - Lancet: Lenalidomide in combination with rituximab for patients with relapsed or refractory mantle-cell lymphoma: a phase 1/2 clinical trial
|
|
|
|
MCL, relapsed - Haematologica: A multicenter phase II trial (SAKK 36/06) of single-agent Everolimus(RAD001) in patients with relapsed or refractory mantle cell lymphoma.
|
|
|
ASH Paper: Len, Benda, and Rituxan As 1st-Line Therapy For Patients >65 Years w Mantle Cell Lymphoma: Prelim Results http://bit.ly/1d2Hls1
Presently, 29 patients are evaluable for response after 6 cycles LBR. ORR is 28/29 (97%), CR+CRu 23 (79%). 17 out of 28 evaluable patients (61%) were MRD- negative after 6 cycles. After a median follow-up of 18 months, the median PFS has not been reached, and the estimated PFS at 2 years is 74%.
|
|
MCL - Haematologica. 2010 August; Front-line treatment of mantle cell lymphoma
|
|
MCL - JCO, 2009: Immunochemotherapy and Autologous Stem-Cell Transplantation for Untreated Patients With Mantle-Cell Lymphoma: CALGB 59909
"There is no clear plateau in the PFS curve, so it remains to be seen if any patients are cured with this treatment. The only proven potential cure for MCL at this time remains allogeneic hematopoietic stem-cell transplantation. 36"
|
|
MCL - ASH. 2006: Reduced-Intensity Regimens in Allogeneic Stem-Cell Transplantation for Non-Hodgkin Lymphoma and Chronic Lymphocytic Leukemia
|
|
MCL - Cancer: Post-treatment (not interim) PET scan status is highly predictive of outcome in mantle cell lymphoma patients treated with R-HyperCVAD
Also see http://1.usa.gov/trRECZ
|
|
MCL - Pub Med: Indolent mantle cell leukemia: a clinic-pathological variant characterized by isolated lymphocytosis, interstitial bone marrow involvement, kappa light chain restriction, and good prognosis
|
|
MCL - Weill Cornell, Dr. Martin: Update from ASH 2011: New treatments for mantle cell lymphoma are on the horizon
|
|
 MCL -Weill Cornell, Dr. Martin: Update from ASH 2011: Rituximab improves survival in patients with mantle cell lymphoma MCL -Weill Cornell, Dr. Martin: Update from ASH 2011: Rituximab improves survival in patients with mantle cell lymphoma
|
|
MCL - Blood: Addition of rituximab to chemotherapy alone as first-line therapy improves overall survival in elderly patients with mantle cell lymphoma
|
|
MCL – Cancer, 2010: Durable Responses with the Metronomic (low daily dose) RT-PEPC in Elderly Patients with Recurrent Mantle Cell Lymphoma
|
|
Prognostic Index Predicts Survival for Patients With MCL Autologous Stem-Cell Transplantation
|
|
Lugano Conference: Rituximab + Lenalidomide Prolonged Remission in Mantle Cell Lymphoma http://bit.ly/lVhZmJ
|
|
Rituxan maintenance: EHA 2011: Remission duration of lymphoma doubled
"Clinical research has shown that recurrence of Mantle Cell Lymphoma, a variant of malignant lymphoma, can be reduced by almost 50% in patients who receive maintenance treatment with the antibody rituximab. These results are presented by Dr Hanneke Kluin-Nelemans at the 16th Congress of the European
Hematology Association in London."
Also see Medcape item: http://www.medscape.com/viewarticle/744453
|
|
The Mantle Cell Lymphoma Prognostic Index (MIPI) Superior to IPI http://bit.ly/5UsntE | Full
|
|
A new prognostic index (MIPI) for patients with advanced stage mantle cell lymphoma. Blood. 2007 Oct 25 PMID: 17962512
According to the MIPI, patients were classified into low risk (44% of patients, median OS not reached), intermediate risk (35%, 51 months), and high risk groups (21%, 29 months), based on the four independent prognostic factors: (1) age, (2) ECOG performance status, (3) LDH and leukocyte count.
|
|
Ki-67 as a prognostic marker in MCL—consensus guidelines of the pathology panel of the European MCL Network ncbi.nlm.nih.gov
|
|
High Rate of Durable Remissions After Treatment of Newly Diagnosed Aggressive Mantle-Cell Lymphoma With Rituximab Plus Hyper-CVAD Alternating With Rituximab Plus High-Dose Methotrexate and Cytarabine. ASCO 2005
|
|
Mantle cell lymphoma: prognostic capacity of the
Follicular Lymphoma International Prognostic Index (FLIPI).
Br J Haematol. 2006 Apr;133(1):43-9. PMID: 16512827 | See FLIPI
|
|
Allogeneic stem cell transplantation for mantle cell lymphoma--does it deserve a better look? Leuk Lymphoma. 2005 Feb;46(2):217-23. PMID: 15621804
|
|
The Leukemic Presentation of Mantle-cell Lymphoma: Disease Features and Prognostic Factors in 58 Patients. Leuk Lymphoma. 2004;45(10):2007-2015. PMID: 15370245
"This analysis demonstrates that except for splenomegaly, survival of MCL patients presenting with leukemia is not significantly influenced by clinical or tumor characteristics. Splenectomy is a useful treatment option in this group of patients."
|
|
Allogeneic “Mini” Stem Cell Transplant Effective for Recurrent Mantle Cell Lymphoma cancerconsultants.com
|
|
Long-term follow-up of autologous stem cell transplantation in patients with diffuse mantle cell lymphoma in first disease remission: the prognostic value of beta2-microglobulin and the tumor score. Cancer. 2003 Dec 15;98(12):2630-5.
PMID: 14669282 | Related articles
|
|
Survivin Expression in Mantle Cell Lymphoma I ... The role of survivin in the pathogenesis of mantle cell lymphoma (MCL) was examined in a series of typical and blastoid tumors. amjpathol.org
|
|
|