|
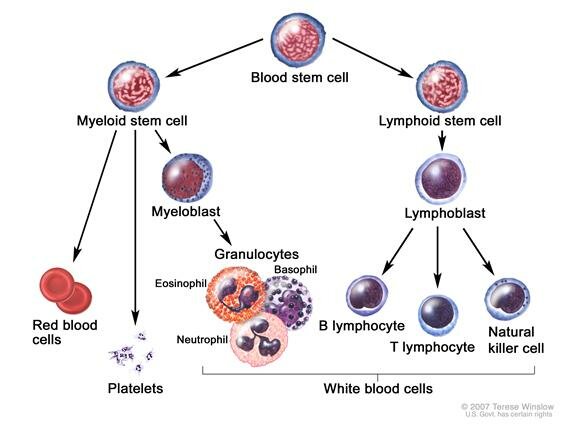
The origin of blood cells - click to enlarge
How to treat myelosuppression?
The treatment for myelosuppression depends on the underlying cause and the type of blood cell involved (see below.) For persistent myelosuppression, obtaining tissue from the bone marrow might be required in order to diagnose the cause. When related to treatment, for example, the condition can resolve in days, weeks, or months after treatment is withheld. When it is caused by the the disease, treating the lymphoma will often resolve the condition. Sometimes biologic growth factors, such as Neupogen, are used to induce the body to produce more blood cells. It might also be helpful to include quality proteins in your diet, B12 and folic acid to give your body the nutrients it needs to produce blood cells. Steroids may help if the neutropenia is caused by an autoimmune reaction.
Resources
|
Side Effects > Low Blood Counts (Myelosuppression)
Last update: 03/14/2014
|
|
TOPICS
Low Blood Counts: Myelosuppression | Cytopenia | Myelodysplastic Syndrome |
Comparing Blood Cells
Related topics: Low Blood Counts
 Myelosuppression is an overall suppression of the blood cells - red blood cells, platelets, and white cells, such as neutrophils and lymphocytes - that are produced in the bone marrow. Myelosuppression is a common side effect of chemotherapy and radiotherapy. It can also indicate that lymphoma is present in the bone marrow. Myelosuppression is an overall suppression of the blood cells - red blood cells, platelets, and white cells, such as neutrophils and lymphocytes - that are produced in the bone marrow. Myelosuppression is a common side effect of chemotherapy and radiotherapy. It can also indicate that lymphoma is present in the bone marrow.
Some causes of myelosuppression:
Cancer, allergic disorders, chemo drugs and radiation, some types of infections, Myelodysplastic syndrome (MDS), autoimmune disease, deficiencies in vitamin B12 and folic acid, insecticides and toxins, and some hereditary diseases. - adapted from Merck.com
MDS is an uncommon but potentially serious side effect of treatment. "The treatment options for MDS depend most on how the bone marrow appears. It is important to be able to predict the likelihood of the MDS transforming into AML given that different, less aggressive treatments are available for MDS that is less aggressive."
~ Dr. Furman's comment (CLL/SLL support group, 8/2010.)
Cytopenia - describes a deficiency in some cellular elements in the blood. There are three classes of cells that are produced in the bone marrow: red blood cells, white blood cells, and platelets.
|
.gif) |
Hypersplenism as cause of cytopenia (low WBC) Merck
"Hypersequestration of blood in a large spleen is the predominant mechanism for cytopenia..."
|
|
White Blood Cell Disorders Merck Manual
Discusses various kinds of white cell disorders and causes.
|
|
About CBC Lab Test Results PAL
|
|
Understanding your Complete Blood Count, neupogen.com PDF - PDF-Help
|
|
Biologics for the treatment of myelosuppression Lymphomation.org
|
|
|
Myelodysplastic Syndrome
 Treatment TOPIC SEARCH: PubMed | ASCO | Medscape | Web Treatment TOPIC SEARCH: PubMed | ASCO | Medscape | Web
"Myelodysplasia encompasses a heterogeneous [varied] group of disorders that result in ineffective hematopoiesis [formation of blood cells].
Historically, a wide variety of terms has been used to describe these syndromes, including preleukemia, refractory anemia with excess of myeloblasts, subacute myeloid leukemia, oligoleukemia, odoleukemia, and dysmyelopoietic syndromes.
The Myelodysplasia syndromes (MDS) are *clonal stem cell disorders* characterized by progressive cytopenia or cytopenias [too many or too few blood cells], usually in the presence of a hypercellular bone marrow and multilineage dysplasia [different classes of abnormal cells].
...
Treatment-related myelodysplasia syndrome following cytotoxic chemotherapy is of more concern in the pediatric population as more childhood malignancies are cured.11 The most common association is with prior alkylator therapy, with or without concomitant radiation. The risk of myelodysplasia syndrome peaks 5-7 years after alkylator treatment and is related to cumulative dose. A strong association with monosomy 7 or del7q is recognized."
Source: emedicine.com
In the News:
|
MDS/ALL: FDA Approves Vidaza medicalnewstoday.com
|
|
Am J Med. 2012 Jul;125(7 Suppl):S18-23. doi:
Myelodysplastic syndromes: therapy and outlook. ncbi.nlm.nih.gov
In patients who are ineligible for potentially curative hematopoietic stem cell transplantation (HSCT), approved therapies such as lenalidomide, azacitidine, and decitabine are available for those who previously would have received supportive care alone. Each treatment can achieve hematologic improvement and enhance quality of life. Azacitidine is the only treatment to show a significant survival advantage in patients with higher-risk MDS compared with conventional care regimens.
|
MDS Resources:
|
Review article on MDS asheducationbook.org
|
|
Myelodysplasia Syndromes, Key Points by NCI 2014:
|
A type of cancer in which the bone marrow does not make enough healthy blood cells and there are abnormal (blast) cells in the blood and/or bone marrow.
|
|
The different types of MDS are diagnosed based on certain changes in the blood cells and bone marrow.
|
|
Age and past treatment with chemotherapy or radiation therapy affect the risk of a MDS.
|
|
Possible signs of a MDS include feeling tired and shortness of breath.
|
|
Tests that examine the blood and bone marrow are used to detect (find) and diagnose MDS.
|
|
Certain factors affect prognosis and treatment options.
|
|
|
Myelodysplasia and acute myeloid leukemia following therapy for indolent lymphoma
with fludarabine, mitoxantrone, and dexamethasone (FND) plus rituximab and interferon alpha pubmedcentral.nih.gov7
|
|
Therapy-Related Myelodysplastic Syndrome: Morphologic Subclassification
May Not Be Clinically Relevant Posted 02/22/2007 medscape.com/ (free login req.)
"The average latency period from onset of therapy for the primary disorder to the development of bone marrow dysfunction was 62 months for t-MDS and 63 months for t-AML. The latency period was not different between patients with primary hematologic malignancies and nonhematologic malignancies, nor was it different among patients who received chemotherapy only, radiotherapy only, or combined modality therapy."
|
|
PLWC Guide to Myelodysplastic Syndromes PLWC (fixed 12/12)
People Living with Cancer (a division of ASCO)
|
|
Clinical Data From REVLIMID(R) Study in Myelodysplastic Syndromes
Reported in NEJM prnewswire.com
"The recent clinical data from this Phase II study evaluating REVLIMID as an oral MDS treatment not only demonstrates hematologic response, but this is the first MDS treatment to demonstrate this level of cytogenetic response." said Dr. Alan List, Professor of Oncology and Medicine, and Chief, Malignant Hematology Division at the H. Lee Moffitt Cancer Center.
|
|
ASCO 2005 - MDS Hematologic and Cytogenetic (CTG) Response to Lenalidomide
(CC-5013) in Patients with Transfusion-Dependent (TD) Myelodysplastic Syndrome (MDS)
and Chromosome 5q31.1 Deletion: Results of the Multicenter MDS-003 Study.
"highly effective in MDS pts with del5q31 with unprecedented hematologic and
CTG remitting activity."
|
|
Vidaza (azacitidine), a new drug to treat MDS, a bone marrow disease that can occur
as a side effect of cancer treatment FDA.org
|
|
According to a recent article published in the Journal of Clinical Oncology, "mini"
allogeneic stem cell transplants may provide a chance for a cure for patients over 60 years of
age with poor-prognosis myeloid (blood) malignancies. cancerconsultants.com
|
|
Specific Regimen [FND] Influences Risk of Myelodysplasia After Lymphoma Treatment
Oncolink
|
|
ASH 2007 report on MDS Oral Glutathione Analogue TLK199 Safe and Effective in Patients With MDS
|
|
Comparing Blood Cells
|
|
White Cells
|
Red Cells
|
Platelets
|
Technical names
|
Neutrophils
Lymphocytes
Monocytes |
Erythrocytes |
Platelets |
Function
|
Fight infections |
Carry oxygen to cells |
Stops bleeding |
Shortage called
|
Neutropenia
|
Anemia
|
Thrombocytopaenia
|
Normal count
|
Total white cells:
4-11(x109/l)
Neutrophils:
2-8 (x106/l)
|
Adult male:
4.4-6 (x1012/l)
Adult female:
4.2-5.4 (x1012/l)
|
130-400 (x109/l) |
Shortage may mean
|
infections |
pale, tired,
breathless, cold, dizzy and having headaches |
Bruising easily
Bleeding longer
Bleeding nose and gums
Blood in urine |
Action See Biologics
|
Antibiotics
Delaying treatment until white count returns to normal
Drugs: Neupogen, Leukine
Also see bcccancer.bc
|
Red cell transfusion
Drug: Erythropoietin
|
Platelet transfusion
Drug: Neumega
|
|
|