TOPIC SEARCH: PubMed | ASCOpost TOPIC SEARCH: PubMed | ASCOpost
About Rituxan Maintenance AshEducationBook
Maintenance perspectives - when and how much?
.gif) |
2017 Opinion: Maintenance Therapies in Indolent Lymphomas:
should Recent Data Change the Standard of Care? http://bit.ly/2vUCPwx
|
|
Pros and cons of rituximab maintenance in follicular lymphoma. - Abstract - Europe PMC http://bit.ly/2to7CTA
Zhang L 1 , Ghielmini M 2 , Cheson BD 3 , Ujjani C
"In summary, most studies have demonstrated a significant benefit in progression-free or event-free survival in this notoriously recurrent disease; however, long-term outcomes could not consistently demonstrate to be improved with this intervention. In a meta-analysis of randomized trials overall survival (OS) showed a tendency to improvement when given to patients in relapse, but no single study reached a significant OS advantage. The risk of high-grade transformation does not seem to be reduced in prospective trials.
On the other hand, MR clearly increases toxicity without an improvement in quality of life. Finally, MR is expensive, and it is not proven that the delayed relapse time can compensate for these costs. In conclusion, despite the proven increase in progression-free survival, MR can't be recommended as a standard for the treatment of FL."
|
|
2016: Dr. Zelenetz on use of Rituxan - For what indications? How much is too much?
https://youtu.be/LY9Ls64M-ak
|
|
ASH Paper: Rituximab Maintenance For a Max Of 5 Years In Follicular Lymphoma: Randomized Phase III Trial SAKK 35/03 http://bit.ly/1b17YL7
Comment: It seems that the favorable part of analysis was done on a subset because of unexpected relapses early in the maintenance arm .. but after adjusting for that (reasonable because treatment was identical at that point) there was no difference in OS (equally good) and toxicities (infection) appears to favor observation.
There is no significant difference in OS and in the observed best response. Maintenance treatment was stopped due to unacceptable toxicity in no patient in arm A vs. 3 in arm B. ... One infection grade ≥3 was reported in arm A whereas 7 infections grade ≥3 occurred in 5 patients in arm B (prolonged maintenance for a maximum of five years).
So we seem to be where we are with PRIMA ... better PFS but with tradeoffs (infection and potential negative impact on subsequent therapy) and no difference in OS at this point.
Regarding the study design: 270 patients (median age 57 years: range 25-82) with either untreated, relapsed, stable or chemotherapy resistant follicular lymphoma of all grades were treated
I have only basic training (novice-level) in statistics as it relates to study design, but results like this suggest that sample size has to be larger in FL studies to account better for biologic variants of FL - especially when the treatment history for eligible patients varies.
One school of thought is that it's not useful to do a clinical study that cannot provide a reliable answer to the primary question because of the design. Increasingly, we face this problem -- an inability to do sufficiently-powered studies because of the limited pool of patients that are willing to enroll in trials. One way to possibly address this problem is to raise the bar - such as requiring a bigger difference in response and duration of response. (KarlS)
|
|
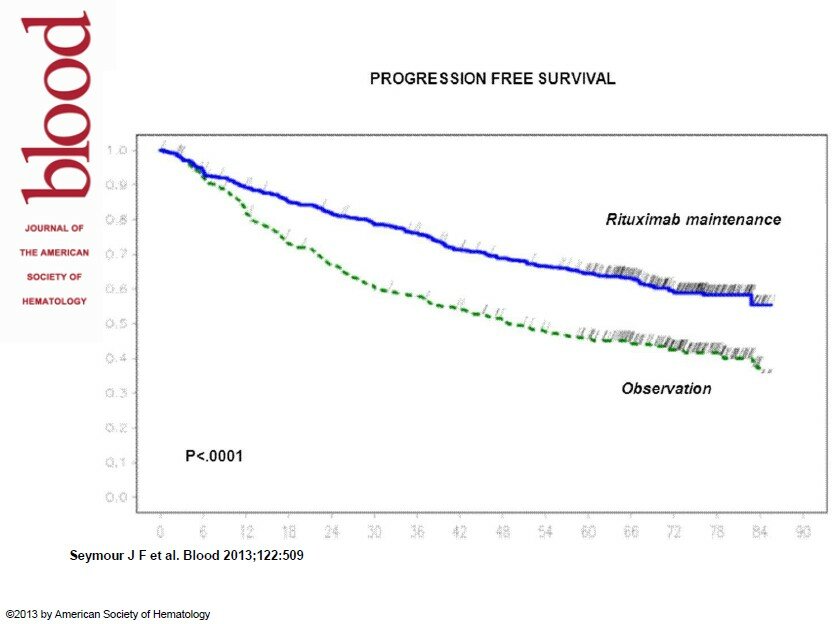
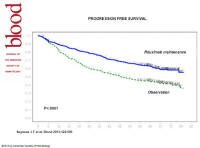
6 Year Follow-Up Of The PRIMA Study of Rituximab Maintenance In previously untreated Follicular Lymphoma Pts following Frontline r-chemo http://bit.ly/1j082j2
COMMENT: It will be interesting to hear the conversation about this report among the experts. My feeling is that this data is more supportive of a benefit for maintenance than the data at 3 years, because the gap in PFS has not narrowed.
Overall response rate to second-line therapy 180/227 (79%) in patients from the observation arm (CR/CRu=61%; PR=19%) versus 109/144 (76%) in patients from the rituximab maintenance arm (CR/CRu =51%; PR=22%) (P=NS). I think the emphasis should be on the CR rate as I feel it's the most clinically important endpoint for subsequent therapy - but even that difference is small.
With a median follow-up of 73 months from randomization, 6-year progression free survival estimate was
42.7% (95% CI 38 – 46.9%) in the observation arm
59.2% (95% CI 54.7 – 63.7%) in the rituximab maintenance arm
|
* J Clin Onc 2013:
Rituximab Maintenance Compared With Observation After Brief First-Line R-FND Chemoimmunotherapy With Rituximab Consolidation in Patients Age Older Than 60 Years With Advanced Follicular Lymphoma: A Phase III Randomized Study by the Fondazione Italiana Linfomi. http://1.usa.gov/13OOMU0
COMMENT: In this study population with abbreviated R-chemo maintenance Rituxan did not provide an advantage in Progression Free Survival (PFS) - however, each group received consolidation with Rituxan (a kind of maintenance) following the R-chemo induction. One might speculate if consolidation with Rituxan would beat two years of maintenance - the controversial standard set by the PRIMA trial.
Overview
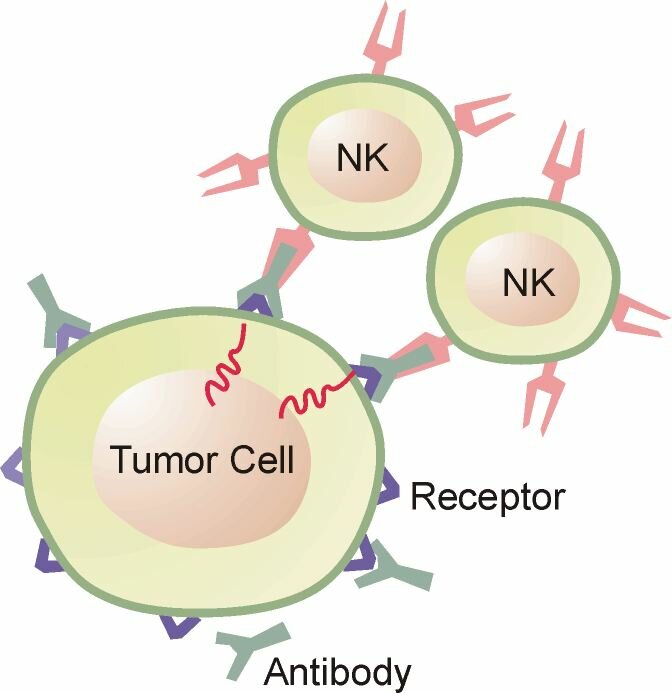
Rituxan Maintenance (RM) is regularly-scheduled-therapy with Rituxan antibody given in weekly cycles. The Rituxan might be given every 3 or 4 months for as long as 2 years for the purpose of increasing the duration of the response to standard therapy for lymphoma, such as Rituxan-based chemotherapy.
Rituxan Maintenance can also be given after single-agent Rituxan therapy.
The potential benefits and risks seem to vary by the type of lymphoma, and by the setting, such as if used for follicular or aggressive lymphoma, after initial therapy, or if used in the relapse setting.
Perspectives on Rituxan Maintenance:
Summary: At this time, some experts favor the use of Rituxan maintenance for follicular lymphoma after first therapy with Rituxan-based chemotherapy, and others do not (see Perspectives that follows and Pros and Cons below). Maintenance Rituxan for Mantle Cell Lymphoma seems to be less controversial because of recent positive findings in a study.
For CLL, maintenance Rituxan is not widely used. Following Rituxan monotherapy, observations appears to be as good as maintenance (based on RESORT) with less cost and toxicity. However, for marginal zone lymphoma a benefit in terms of PFS was found in the RESORT study.
An important question is the reliability of Progression Free Survival (PFS) as a way to measure clinical benefit in the first line setting. PFS is a composite endpoint that counts progression, relapse, or death as one event. Notably, to our knowledge, there has been no significant difference in deaths reported in the studies that have evaluated Rituxan as maintenance compared to observation at this time (April 2013).
Return to top
Tradeoffs: Pros and Cons of Rituxan Maintenance (RM)
for indolent follicular lymphoma after Initial therapy - an advocate's perspective:
Advantages
|
Disadvantages
|
|
Based on the PRIMA study this use of Rituxan for this indication delays time to relapse. CI means confidence interval.
at 2 years: PFS (progression free survival*)
82%; CI [78-86%] for Maintenance vs.
66% CI [61-70%] for observation
at 3 year PFS was
78.6% (CI 74.7 - 82%) maintenance arm vs.
60.3% observation arm (CI 55.8 - 64.5%)
at 6 years: PFS was
59.2% (95% CI 54.7 – 63.7%) maintenance arm 42.7% (95% CI 38 – 46.9%) observation arm
|
|
Rituxan maintenance seems to increase the complete response (CR) rate, which is associated with better long term outcomes
Note: PFS is a composite endpoint counting progression or mortality as an event. In this study PFS is a measure of time to relapse only, because there was no difference in mortality at 2 and 3 years.
|
|
Some of us will be comforted by the closer monitoring we may receive while regular therapy on a regular schedule
|
|
Maintenance increases the odds of having a durable response to first line therapy. Arguably, being in remission without evidence of disease improves the quality of life of the patients during this period of time.
|
|
|
You may be given more treatment than is needed – as 66%, 60%, and 43% where in remission with observation after 2, 3, and 6 years of follow up respectively (PRIMA)
|
|
The extended use of Rituxan may increase your risk for low immunoglobulin (IG) levels with an increase in certain types of infection (sinus, lung);
Low Ig levels may also cause
rare but very serious side effects.
|
|
Regular use of Rituxan may lead to resistance to Rituxan-based treatment when/if treatment is again needed and perhaps (in theory) to radioimmunotherapy, which also targets cd20.
Resistance to Rituxan is a theoretical concern. It might be estimated by comparing responses to subsequent therapy with Rituxan-based therapy.
PRIMA at 6 yr:
Overall response rate (ORR) to second-line therapy was reported as
ORR = 180/227 (79%) in observation arm
(CR/CRu=61%; PR=19%) versus
ORR = 109/144 (76%) in patients from the rituximab maintenance arm
(CR/CRu =51%; PR=22%) (P=NS). "
Arguably, the CR rate (51% vs 61%) is the more important outcome to monitor and compare in order to judge the impact of maintenance on developing treatment resistance to Rituxan-based therapy.
|
|
More treatments may require more monitoring for toxicities and response (increasing the expense)
|
|
Maintenance increases the cost of treatment without a study showing a difference in outcomes in the long term (Overall Survival). There is no difference in OS with 6 years of follow-up (PRIMA).
OS is the most reliable endpoint as it account for all effects - known and unknown.
|
|
Individual factors?
|
Uncertainties:
|
|
How quickly and completely you responded to standard treatment (given just before Rituxan maintenance) could help to decide which is preferable for you.
For example, difficulty with induction therapy, or a slow response, or a response that was not complete might be a reason to choose RM.
A third option in this circumstance (a partial response to r-chemo) is radioimmunotherapy– a study we’d like to see done in a head-to-head method.
|
|
The treatment history seems to matter. The RESORT study gave the advantage to observation for follicular lymphoma when the initial therapy was Rituxan x4; while the PRIMA study gave the advantage to maintenance Rituxan when used after Rituxan-based chemotherapy.
|
|
Personal preference – some patients like the idea of hitting “it” again when it’s down; others prefer “saving bullets.” One’s anxiety level about the chance of the lymphoma returning sooner could be a factor.
|
|
|
Treating with Rituxan or other therapy as needed could be as effective.
It is not yet known if Rituxan maintenance improves survival in the long term. More follow up time is needed in the studies that were done.
An advantage in time to progression does not necessarily predict a benefit in the long term.
|
|
Different schedules of Rituxan maintenance have not been evaluated in a controlled way.
For example, 2 years of maintenance has not been compared to 1 year.
|
|
The rate of histological transformation did not appear to differ between the 2 treatment arms after 6 years of follow up (PRIMA)
|
|
Some subtypes of indolent lymphoma may do better with maintenance Rituxan than others.
See A subgroup analysis of small lymphocytic and marginal zone lymphomas in the Eastern Cooperative Oncology Group protocol E4402 (RESORT): A randomized phase III study comparing two different rituximab dosing strategies for low tumor burden indolent non-Hodgkin lymphoma. asco.org
|
|
|
Patient experiences with Maintenance
|
Return to top
Comment on PFS, a composite endpoint – "rolling three things into one statistic" progression, relapse, and death from any cause.
Re: The sponsor’s website describes the results of PRIMA:
http://www.rituxan.com/hem/hcp/non-hodgkin/post-induction/prima/index.html
My concern is that the sponsor statement will be interpreted by many readers that you have a lower chance of dying with maintenance.
"RITUXAN maintenance provided a 46% reduction in the risk of progression, relapse, or death (p<0.0001)
I feel that the sponsor should add: However, at the time of analysis there was no difference in the death rate between he compared groups.
(Readers may not appreciate the meaning of “or.” )
Regarding the context: For indolent lymphomas we might use the metaphor of a distance run to describe an outcome of treatment. Here an advantage in PFS shows who is doing better after two miles in a 10 – 12 mile run. Noting that what is “spent” early to achieve that advantage can also be used later as needed to help run as far as possible and that it’s not possible to know who needs to use it – who would do as well without it.
So comparing also the duration of a remission from the end of the respective treatment would be informative as a way to estimate if the extra treatment is likely to improve survival – provides clinical benefit. Coming back to the metaphor: This in a race where virtually everyone who started it is still in it (no difference in drop outs after 2 miles). Did the gap between the groups of runners who received MR increase, stay the same, or decrease after the MR was discontinued?
… Intuitively this additional analysis would help to judge if the disease status of the patients at 2 years predicts a survival advantage for those who had the extra treatment. This information would help physicians and patients to make more informed choices.
So I feel this is a consent / truth in advertizing issue – noting that such interpretations of the outcomes appear to have influenced clinical practice. Maintenance R has been widely adopted based on this study (despite some expert disagreement on whether it should be).
(For a dissenting view, see Cheson: Rituximab for Follicular Lymphoma: Maintaining an Open Mind http://bit.ly/mxny1J )
There is another reason for concern and that is that the widespread use of RM in this setting has led to study proposals seeking to build on this –using RM as the backbone and comparator in studies testing new agents for lymphoma.
So I worry that there has been a rush to judgment on the clinical significance of the outcomes in this study. I feel that it needed longer follow up, and could possibly benefit from analysis using other endpoints – such as duration of response from end of therapy. The statement on PFS, while accurate, needs to be clarified in respect to deaths.
Regarding the use of RM, I personally think it’s a close call – reasons for and against maintenance, and patient preference matters (early benefit versus risks of achieving that benefit – and considering that 60% did as well without extra treatment.
The risks of maintenance R (MR) include: rare but fatal PML, serious, more common but not a majority: low Ig antibodies leading to chronic infection.
The uncertainty is if using R as needed is as good with less cost and risk (supported by RESORT study) and if MR will lead to resistance to R when it is eventually needed again Masking a relapse in theory could select for treatment-resistance clones. If true, then the focus of research should be on improving induction therapy which is harder to assess when maintenance is added (was it induction or maintenance the provided the improvement in the endpoint?).
Thanks for listening!
KarlS
Is Progression Free Survival the Right Endpoint for Judging the Clinical Benefit of Maintenance Rituxan following First Therapy for Indolent Lymphoma? An advocate's perspective
Return to top
Reports: Indolent Lymphoma - previously untreated
PRIMA (Maintenance after R-chemo)
|
ASH - December 4, 2010: Updated Results of the PRIMA Study Confirms the Benefit of 2-Years Rituximab Maintenance In Follicular Lymphoma Patients Responding to Immunochemotherapy ash.confex.com/
1217 patients were enrolled from 223 centres
After a median follow-up of 36 months,
3-year PFS (progression free survival) was
60.3% (confidence range 55.8 - 64.5%) in the observation arm and
78.6% (confidence range 74.7 - 82%) in the rituximab maintenance arm
Most common adverse events reported were infections (24% and 39%) in the observation and rituximab maintenance arms respectively. Grade 3-4 adverse events were reported in 17% of patients in the observation arm and 24% in the rituximab maintenance arm (neutropenia 1% vs 4%; infections 1% vs 4%, respectively) but these lead to treatment discontinuation in only 8 and 19 patients, respectively.
|
|
Rituximab maintenance for 2 years in patients with untreated high tumor burden follicular lymphoma after response to immuno-chemotherapy. PRIMA (corrected) study: http://www.asco.org
2-year PFS:
82%; confidence range 78-86% for RM vs
66% confidence range 61-70% for observation
|
RESORT (Maintenance after R monotherapy)
|
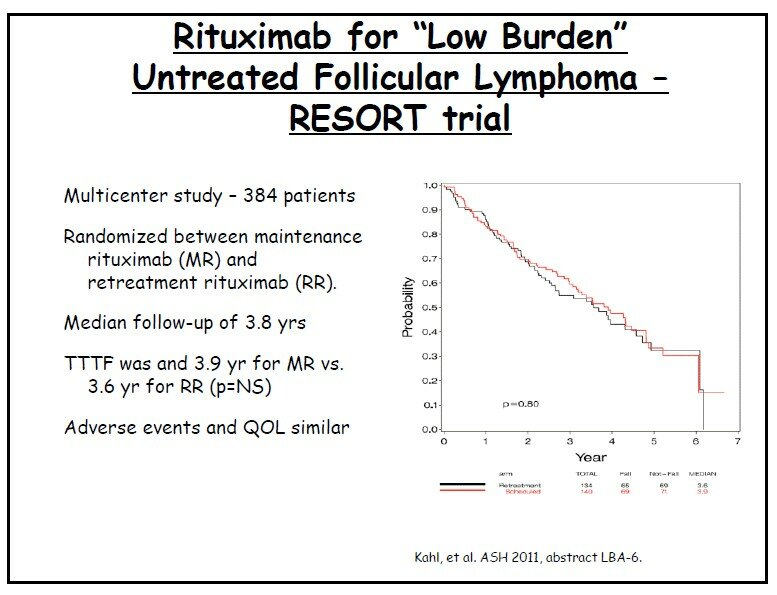
RESORT: A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Follicular Lymphoma http://abstracts.hematologylibrary.org
Comments by PAL:
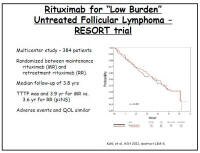 The results (in terms of responses and duration of response) were encouraging with an important finding that giving Rituxan as needed is as good as regularly scheduled maintenance - mitigating some of the risks of this approach (by using less Rituxan) to treating follicular lymphoma when treatment is not yet indicated. The results (in terms of responses and duration of response) were encouraging with an important finding that giving Rituxan as needed is as good as regularly scheduled maintenance - mitigating some of the risks of this approach (by using less Rituxan) to treating follicular lymphoma when treatment is not yet indicated.
Unfortunately the plot of Time to Treatment Failure (TTTF) does not suggest a curative potential for Rituxan monotherapy.
Because there was no observation group as a control, we don't know if the participants with ongoing remissions would have done as well with observation - initiating first treatment when needed.
Does the cited historical comparator of 3 years to first treatment predict the median time to first treatment for those with low tumor burden?
The first treatment might not necessarily be chemotherapy for patients who wait for a need to treat.
Will the early use of Rituxan increase the risks to patients receiving Rituxan-based chemo (such as Ig depletion and associated infections) preclude use of maintenance Rituxan after chemo?
|
|
Less Is More for Rituximab in Low-Burden Follicular Lymphoma
http://www.medscape.com/viewarticle/755445
|
|
ASH: Rituximab Dosing Schemes Prove Equal in Low-Burden FL medpagetoday.com/
"The time to treatment failure was about four years in those patients on a maintenance strategy and for patients on a retreatment strategy upon relapse episodes"
|
|
A subgroup analysis of small lymphocytic and marginal zone lymphomas in the Eastern Cooperative Oncology Group protocol E4402 (RESORT): A randomized phase III study comparing two different rituximab dosing strategies for low tumor burden indolent non-Hodgkin lymphoma. asco.org
" Conclusions: A planned subgroup analysis of non-FL pt showed significant benefit in time to treatment failure (TTTF), and time to first cytotoxic therapy (TTCT) for Maintenance R but with 2 grade 4 toxicities. This differs from the follicular lymphoma pt in this trial, for whom response to induction was higher (70 vs. 41%; p<.0001) and where no TTTF benefit was observed with MR. Low Tumor Burden non-follicular indolent lymphoma pt who achieve a CR or PR to induction R benefit from Maintenance R therapy."
|
Other
|
JCO: Long-Term Follow-Up of Patients With Follicular
Lymphoma Receiving Single-Agent Rituximab at Two
Different Schedules in Trial SAKK 35/98 jco.ascopubs.org.pdf
Patients (prior chemotherapy 138; chemotherapy-naive 64) received single-agent rituximab and if non-progressive, were randomly assigned to no further treatment (observation) or four additional doses of rituximab given at 2-month intervals (prolonged exposure).
|
|
First line Rituxan for CLL:
Single-agent rituximab as first-line and maintenance treatment for patients with chronic lymphocytic leukemia or small lymphocytic lymphoma: a phase II trial of the Minnie Pearl Cancer Research Network. J Clin Oncol. 2003 May 1;21(9):1746-51. PMID: 12721250
|
|
Rituximab as first-line and maintenance therapy for patients with indolent non-hodgkin's lymphoma. J Clin Oncol. 2002 Oct 15;20(20):4261-7. PMID: 12377971 | Related articles
CONCLUSION: Rituximab is highly active and extremely well tolerated as first-line single-agent therapy for indolent NHL. First-line treatment with scheduled maintenance at 6-month intervals produces high overall and complete response rates and a longer progression-free survival (34 months) than has been reported with a standard 4-week treatment.
|
|
Rituximab (anti-CD20 monoclonal antibody) as consolidation of first-line CHOP chemotherapy in patients with follicular lymphoma: a phase II study. Eur J Haematol. 2002 Jul;69(1):21-6. PMID: 12270058 - PubMed
|
Reports: Indolent Lymphoma, Relapse Setting
|
Rituxan following R-FCM in Relapsed follicular NHL: PMID: 16946304
|
|
JCO, 2010: Rituximab Maintenance Treatment of Relapsed/Resistant Follicular NHL: Long-Term Outcome of the EORTC 20981 Phase III Randomized Intergroup Study http://bit.ly/9mVxh5
|
|
Maintenance Rituxan following Relapse of follicular NHL jco.org
|
|
Rituximab long-term maintenance therapy after autologous stem cell transplantation in patients with B-cell non-Hodgkin’s lymphoma springerlink.com
|
|
ASH 2002: Proleukin® Plus Rituxan® may Reduce Recurrences Following Stem Cell Transplant in Non-Hodgkin’s Lymphoma - CancerConsultants.com
|
|
Rituximab maintenance improves clinical outcome of relapsed/resistant follicular non-Hodgkin's lymphoma, both in patients with and without rituximab during induction: results of a prospective randomized phase III intergroup trial. Blood. 2006 Jul 27; PMID: 16873669
|
Reports, Indolent and Relapsed settings
|
Overview of Studies: Rituximab maintenance therapy: a step forward in follicular lymphoma http://bit.ly/9pncbR
|
|
Rituximab Maintenance for the Treatment of Patients With Follicular Lymphoma: Systematic Review and Meta-analysis of Randomized Trials medscape.com (free login req.)
|
|
Follicular lymphoma: chemotherapy and/or antibodies?
Michele Ghielmini ONCOLOGY INSTITUTE OF SOUTHERN SWITZERLAND - http://www.bloodjournal.org/cgi/content/full/108/10/3235
|
|
Extended use of Rituxan in Newly diagnosed and relapsed follicular NHL
Prolonged treatment with rituximab in patients with follicular lymphoma significantly increases event-free survival and response duration compared with the standard weekly x 4 schedule. Blood 2004;. PubMed
Source: http://www.ncbi.nlm.nih.gov
|
Reports, Aggressive Lymphoma, various types and settings
|
LL, 2011: Maintenance rituximab following induction chemo-immunotherapy for mantle cell lymphoma:
long-term follow-up of a pilot study from the Wisconsin Oncology Network. http://www.ncbi.nlm.nih.gov/pubmed/21864042
"These long-term results suggest that the modified R-hyperCVAD regimen with maintenance rituximab is an excellent option for older patients with newly diagnosed mantle cell lymphoma."
|
|
Rituxan maintenance for DLBCL following CHOP-R? ASCO 2007 http://bit.ly/1SkdJX
As 6-yr FFS declined to <50% among R-CHOP responders, with or without MR, there is a need for more effective treatment strategies in older DLBCL pts.
|
Return to top
|