|
Guidelines at Diagnosis | About Clinical Trials |
|
|
evidence-based support and information |
|
|
|
|
Transformation is suspected or indicated by how it behaves (clinical) or by evaluation of a biopsy as described in the following report, ASH 2012: Rates and Outcomes of Follicular Lymphoma Transformation in the Rituximab Era: A Report From the University of Iowa/Mayo Clinic SPORE Molecular Epidemiology Resource Clinical versus histologic criteria for transformation:The following clinical changes raise suspicion of transformation:
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
2016: Poor outcomes for histologically transformed follicular lymphoma warrant use of salvage HSCT http://bit.ly/2e7T0wT
|
|
ASH Ed.: The incidence, natural history, biology, and treatment of transformed lymphomas |
|
Best Pract Res Clin Haematol. 2011, Lossos, Gascoyne:
|
|
BJH (correspondence): Improving survival in patients with transformed B cell non Hodgkin lymphoma: consolidation with Zevalin-BEAM and autologous stem cell transplantation |
|
Clinical Trials for Transformed lymphoma:
|
|
Stem cell mimicry: key to lymphoma transformation? http://bit.ly/2bTkKc |
|
When an indolent lymphoma transforms only some of the malignant cells become aggressive. Generally, the goal of therapy is to cure the transformed cells, but the indolent cells may survive this therapy. |
|
A transformation of CLL is called Richter's syndrome, which is less common than the so-called histologic transformation of follicular lymphoma. |
|
|
When the growth rate becomes rapid, some experts recommend treating it as if it was a histological transformation, whether it has been confirmed by biopsy or not. Consider that a biopsy is only a small sample of what exists, so only on positive finding is conclusion ... there could be transformed cells in another area. |
|
|
It seems that no single test is conclusive for transformation, with the exception of a positive finding from a biopsy. That is, there can sometimes be clinically apparent instances of transformation despite unsuspicious LDH, PET values, etc. |
|
|
If the clinical behavior of the indolent lymphoma becomes aggressive the approach to treatment changes. You typically treat with intent to cure the transformed (aggressive) component, as you would a de novo (primary) aggressive lymphoma (NCCN 2011). |
|
Pathologic confirmation from a tissue sample - a biopsy Adapted from oncolink.org | PubMed | PMID 18838711 | Cancer.gov |
Genes are the "recipes" for proteins that determine cell behavior. The lymphoma cells can acquire additional genetic mutations that alter the growth rate, growth pattern, and sometimes sensitivity to treatment. When it's a confirmed histological transformation, the change is apparent as a new growth pattern: diffuse instead of nodular.
Transformation of indolent lymphoma to faster growing (aggressive) grade of the disease is
common during the course of the disease."Patients with indolent lymphoma may experience a relapse with a more aggressive histology. If the clinical pattern of relapse suggests that the disease is behaving in a more aggressive manner, a biopsy should be performed.
Documentation of conversion to a more aggressive histology requires an appropriate change to therapy applicable to that histologic type.
Rapid growth or discordant growth between various disease sites may indicate a histologic conversion.
"Histologic conversions should be treated with the regimens described in the Aggressive, Recurrent Adult Non-Hodgkin's Lymphoma section of this summary. The durability of the second remission may be short, and clinical trials, should be considered." Cancer.gov
Risk Factors for Early Transformation of Follicular Lymphoma:
Report From the National LymphoCare Study (NLCS) http://bit.ly/5KN44NTechnical:
Transformation of follicular lymphoma to DLBCL proceeds
by distinct oncogenic mechanisms http://bit.ly/8Sx0e1Determinants of the optimal first-line therapy for follicular lymphoma:
A decision analysis http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2932442/
cites this report:
Population-based analysis of incidence and outcome of transformed NHL.
http://www.ncbi.nlm.nih.gov/pubmed/18838711
when saying: "In the largest population-based series of 600 patients, the annual risk
of transformation was estimated to be 3% per year, and the median survival after
transformation was 1.7 years [13].
In subset analysis (denominator not specified), the annual risk of transformation after anthracycline/radiation-based therapy was 1.5%, compared to 3% after alkylator/purine-based therapy.
|
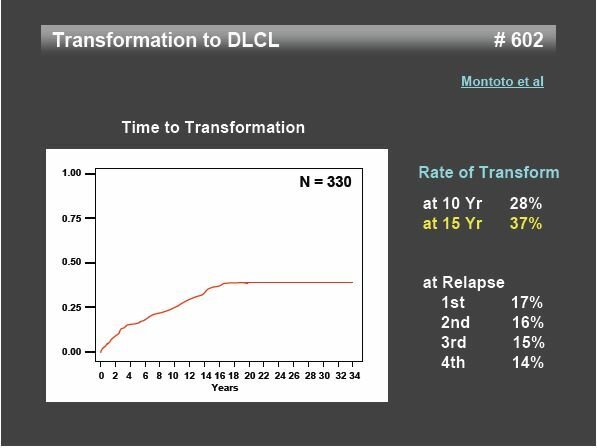
The risk of histologic transformation (HT) by 10 years was 28%. 1 |
|
|
Transformation to more aggressive large cell lymphoma occurs in 25-60% of pts with FL 4 |
|
|
Rate of Transform |
at 10 Yr 28%
at 15 Yr 37%
Click chart to enlarge it
Source: hememalignancies.com pdf
2016, June: Risk Factors and Outcomes for Patients With Follicular Lymphoma Who Had Histologic Transformation (HT) After Response to First-Line Immunochemotherapy (rituxan-chemo) in the PRIMA Trial PDF full report
|
|
Nov 2015:
|
|
Aug 2015:
|
|
Blood 2015: Casulo, Burack, Friedberg
|
|
Blood 2014:
|
|
Blood 2013:
|
|
ASCO Post, 2012: : Predictors and Treatment for Transformed Lymphoma: Current Paradigms http://bit.ly/12V268Z"To date, it is unclear whether early treatment vs a “watch and wait” strategy has any impact on the risk of transformation. Most studies suggest there is no change in risk. |
|
ASCO POST, May 2013: Role of Stem Cell Transplantation in [transformed] Follicular Lymphoma ascopost.com
|
|
ASCO POST, May 2013:
|
|
|
ASCO 2013: Changes in the tumor microenvironment associated with transformation in follicular lymphoma. |
*Blood 2013:
|
|
ASCO Post, 2012: : Predictors and Treatment for Transformed Lymphoma: Current Paradigms http://bit.ly/12V268Z"To date, it is unclear whether early treatment vs a “watch and wait” strategy has any impact on the risk of transformation. Most studies suggest there is no change in risk. |
|
ASCO POST, May 2013: Role of Stem Cell Transplantation in [transformed] Follicular Lymphoma ascopost.com
|
|
ASCO POST, May 2013:
|
|
|
ASCO 2013: Changes in the tumor microenvironment associated with transformation in follicular lymphoma. |
ASH 2012: Rates and Outcomes of Follicular Lymphoma Transformation in the Rituximab Era: A Report From the University of Iowa/Mayo Clinic SPORE Molecular Epidemiology Resource |
|
ASH Ed: The incidence, natural history, biology, and treatment of transformed lymphomas |
|
An international phase II trial of single-agent lenalidomide for relapsed or refractory aggressive B-cell non-Hodgkin’s lymphoma http://annonc.oxfordjournals.org/content/22/7/1622.short
|
|
Gene Expression Signature of Host Immune Response Is Predictive of Follicular Lymphoma Patient Survival in Independent Cohorts, and Correlates with Transformation to Diffuse Large B-Cell Lymphoma ASH 2009 |
|
High rate of survival in transformed lymphoma after autologous stem cell
|
n = 56 "select" patients with transformed lymphoma (25) or de novo DLBCL (25)
Comment: encouraging news given the prognosis of transformed lymphoma, but the study is small (n = 25 transformed) and the participants were selected by investigators using unspecified criteria ... key factors such as age and having chemo-sensitive disease, untreated/previously treated, etc. were not described in the abstract.
Population-based analysis of incidence and outcome of transformed NHL.
Al-Tourah AJ, Gill KK, Chhanabhai M, Hoskins PJ, Klasa RJ, Savage KJ,
Sehn LH, Shenkier TN, Gascoyne RD, Connors JM.
J Clin Oncol. 2008 Nov 10;26(32):5165-9. Epub 2008 Oct 6. PMID: 18838711
n = 600 patients with newly diagnosed FL met the inclusion criteria.
Conclusion: The annual risk of transformation of FL is 3% continuing without plateau beyond 15 years.
Advanced stage at diagnosis is predictive of future transformation.
Clinically diagnosed transformation* has an equal impact on outcome as biopsy proven transformation.
"advanced stage (III, IV, or I/II with B symptoms or bulky disease)
was predictive for the development of transformation (P.002)."
Patients with limited extent transformation had a significantly better
survival with a 5-year post-transformation survival of 66%.
[supporting careful, regularly scheduled monitoring; timely reporting of symptoms by patients]
Patients requiring multiple courses of therapy appear to be at significantly higher risk of transformation
Confounder: 87% of this population were not treated with R-based chemo at transformation
(before introduction of Rituxan) Patient selection: 1986 - 2001
Transformation of follicular lymphoma: prognostic factors and effect on survival
ASCO
Conclusions: prognostic factors for TF include lack of CR, elevated LDH, and B symptoms.
TF is associated with a higher risk of death than FH without TF at first and subsequent
relapses; however, time to TF does not affect long term survival.The Follicular Lymphoma International Prognostic Index (FLIPI) and the histological
subtype are the most important factors to predict histological transformation in
follicular lymphoma PDF
Conclusion: FLIPI and histology were the most important variables predicting HT. Upon HT,
only patients achieving CR (complete response) reached prolonged survival,
thus emphasizing the need for effective therapies once this event occurs.Feasibility of allogeneic stem cell transplantation for follicular lymphoma undergoing
transformation to diffuse large B-cell lymphoma.
Leuk Lymphoma. 2008 Oct;49(10):1893-8. PMID: 18949613
n = 8 patients with histologically confirmed transformation to diffuse large B-cell lymphoma
underwent HSCT at our institution. The median age was 56 years (range 44-63 years).
Allogeneic HSCT appears feasible in patients with transformed FL and is associated with
acceptable treatment-related mortality and low relapse rates.The impact of initial treatment of advanced stage indolent lymphoma on the
risk of transformation ascopubs.org
n = 698 patients with indolent NHL, no prior treatment, age16–60 y and advanced stage disease
(III/ IV or I/ II with B symptoms or bulky disease 10cm).
"Conclusion: The use of an anthracycline-based regimen as initial treatment for advanced stage indolent NHL is associated with a marked reduction in the risk of future transformation."
Modern Pathology (2007) 20, 63–75. doi:10.1038/modpathol.3800708; published online 29 September 2006
The impact of initial treatment of advanced stage indolent lymphoma on the risk of transformation ascopubs.org
|
|
Risk and Clinical implications of Transformation of Follicular Lymphoma to Diffuse Large B-cell Lymphoma (Single Center Experience) JCO.org
The diagnosis of transformation was made in 88 patients at a median of 3 years (range, 0.1 to 16.2 years). Among these 88 patients, 14 transformed before initiation of any therapy (two within 3 months of diagnosis) and 10 during initial therapy. ...
|
|
The Follicular Lymphoma International Prognostic Index (FLIPI) and the histological subtype are the most important factors to predict histological transformation in follicular lymphoma (Single Center experience) annonc.oxfordjournals.org
|
|
Gene-Expression and Immunohistochemical Study of Specific T-Cell Subsets and Accessory Cell Types in the Transformation and Prognosis of Follicular Lymphoma. J Clin Oncol. 2007 Jan 2; PMID: 17200149 | Related articles |
|
The International Prognostic Index predicts outcome after histological transformation of low-grade non-Hodgkin lymphoma. Leuk Lymphoma. 2006 Sep;47(9):1794-9. PMID: 17064990 |
|
Molecular pathogenesis of follicular lymphoma: a cross talk of genetic and immunologic factors. J Clin Oncol. 2005 Sep 10;23(26):6358-63. Review. PMID: 16155020 |
|
A Proteomic Approach to Discovery of Candidate Proteins Involved in the Transformation of Follicular Lymphoma ASH 2005 |
|
Long-term survival after histologic transformation of low-grade follicular lymphoma. J Clin Oncol 13 (7): 1726-33, 1995. Full Text |
|
Transformed lymphoma: an Achilles' heel of non-Hodgkin's lymphoma.
|
|
Incidence, predictive factors, and outcome of lymphoma transformation in follicular lymphoma patients. J Clin Oncol. 1997 Apr;15(4):1587-94. PMID: 9193357 | Related |
|
Follicular lymphoma: prognostic factors for response and survival - Journal of Clinical Oncology, Vol 4, 1470-1480 abstract |
|
International Prognostic Index (IPI) Predicts Outcome after Histological Transformation of Low Grade Non-Hodgkin Lymphoma. Reader-friendly |
|
Long-term survival after histologic transformation of low-grade follicular lymphoma. J Clin Oncol. 1995 Jul;13(7):1726-33. PMID: 7602362 PubMed | Related |
|
Histological conversion of follicular lymphoma with structural alterations of t(14;18) and immunoglobin genes. Leukemia. 1995 Oct;9(10):1748-55. PMID: 7564520 PubMed | Related abstracts
|
|
Large-cell transformation of chronic lymphocytic leukemia and follicular lymphoma during or soon after treatment with fludarabine- rituximab- containing regimens: natural history- or therapy-related complication? Eur J Haematol. 2002 Feb;68(2):80-3. PMID: 12038452 PubMed | Related |
|
Prognostic value of chromosomal abnormalities in follicular lymphoma. Blood. 1994 Aug 15;84(4):1043-9. PMID: 8049424 PubMed | Related |
|
Acute liver failure as initial manifestation of low-grade non-Hodgkin's lymphoma transformation into large-cell lymphoma. Leuk Lymphoma. 2001 Jul;42(3):555-9. PMID: 11699425 PubMed | Related |
|
Transformation of follicular lymphoma: prognostic factors and effect on survival Year: 2002 Abstract No: 1129
|
|
An autopsy study of histologic progression in non-Hodgkin's lymphomas. 192 cases from the National Cancer Institute. Cancer. 1983 Aug 1;52(3):393-8. PMID: 6344979 PubMed | Related |
The Tumor Microenvironment Measured by Flow Cytometry Predicts Overall Survival (OS) and Transformation Risk (TR) in Follicular Lymphoma. Session Type: Poster Session, Board #584-II ASH 2006
|
|
Fine-needle aspiration in non-Hodgkin lymphoma: evaluation of cell size by cytomorphology and flow cytometry. Am J Clin Pathol. 2002 Jun;117(6):880-8. PMID: 12047139 PubMed | Related abstracts |
Reports consistently show that achieving a complete response (CR) is essential to long term survival (PMID: 16940035)
How that is best achieved depends on many factors and so you must consult with your oncologist, preferably a lymphoma expert, on which of the many protocols are most appropriate to your age, treatment history, performance, and so on.
It appears that patients with no initial therapy, or who have achieved a CR from initial therapy, have a more favorable prognosis.
What is most often prescribed for transformed follicular is CHOP-R, but reports indicate that Bendamustine and radioimmunotherapy (RIT) can also be effective against transformed disease.NEWS:
Lenalidomide (LEN) in patients with transformed lymphoma: Results from a large international phase II study (NHL-003). http://bit.ly/a234dx
"LEN has promising clinical activity and achieves durable responses in patients with TL. Also, it may be necessary to consider the original histology when setting a course of therapy for patients with TL. Further studies are needed in this hard-to-treat population."
Note: there's no sure-fire way to query ClinicalTrials.gov to find trials that are open to patients with transformed lymphoma. Some trials exclude patients with this status, others include in the CONDITION field, but many studies don't specify one way or the other. Here are three such studies that may be open and reasonable tries for relapsed transformed FL - that are not transplant:
* Testing DCDT2980S OR DCDS4501A (antibody - drug conjugates) WITH Rituxan http://1.usa.gov/SppweO
* Testing: ABT-199 WITH Bendamustine-Rituximab http://1.usa.gov/10StJaU
* Testing: Everolimus WITH Rituxan maintenance AFTER High-dose Consolidative Therapy http://1.usa.gov/V8CeiG
What protocol would you recommend if the lymphoma is not chemosensitive? |
|
Is following chemotherapy with Radioimmunotherapy (bexxar / zevalin) indicated? |
|
Is it advisable to use PET to determine response to treatment early, so you can change the protocol if needed as early as possible? |
|
Is high dose therapy with stem cell rescue indicated? |
|
What clinical trial protocols look promising for transformed lymphoma? |
|
What is the rationale for the recommended treatment? |
Pivotal Study of Iodine I 131 Tositumomab for Chemotherapy-Refractory Low-Grade or Transformed Low-Grade B-Cell Non-Hodgkin’s Lymphomas http://jco.ascopubs.org |
|
Randomized Controlled Trial of Zevalin Versus Rituximab Immunotherapy for Patients With Relapsed or Refractory Low-Grade, Follicular, or Transformed B-Cell NHL http://bit.ly/aoKHyQ |
|
Multicenter Phase II Study of Bexxar for Chemotherapy-Relapsed/Refractory Low-Grade and Transformed Low-Grade B-Cell NHL http://bit.ly/aX3cZf
|
|
Bexxar and Transformed disease? ASCO | Full text http://theoncologist.alphamedpress.org/cgi/content/full/9/2/160 |
|
Zevalin and Transformed disease? ASCO |
|
The Follicular Lymphoma International Prognostic Index (FLIPI) and the histological subtype are the most important factors to predict histological transformation (HT) in follicular lymphoma (Single Center Experience) annonc.oxfordjournals.org
|
|
Risk and Clinical Implications of [Histologic] Transformation (HT) of Follicular Lymphoma to Diffuse Large B-cell Lymphoma (Single Center Experience) jco.org
|
|
Meet the Professors - a provocative discussion among experts regarding first treatment options for advanced follicular lymphoma, including indications of transformation meettheprofessors.com |
|
High-dose therapy and autologous stem-cell support for chemosensitive transformed low-grade follicular non-Hodgkin's lymphoma: a case-matched study from the European Bone Marrow Transplant Registry. J Clin Oncol 19 (3): 727-35, 2001. PuMed |
|
Deregulation of the Insulin-Like Growth Factor Type 1 Receptor (IGF-1R) in Transformed Follicular Lymphomas: Implications for Novel Therapy. ASH 2006
|
|
Auto-transplants for histologically transformed follicular non-Hodgkin's lymphoma related abstracts |
|
Aggressive NHL: Oncology Board Review Manual yr 2000 PDF |
|
Overview Aggressive Non-Hodgkin's Lymphomas Lymphoma InfoNet |
|
High-dose therapy with autologous haematopoietic support in patients with transformed follicular lymphoma: a study of 27 patients from a single centre. Ann Oncol. 1998 Aug;9(8):865-9. PMID: 9789609 PubMed |
|
Autologous peripheral blood progenitor cell transplantation for transformed diffuse large-cell lymphoma. Clin Lymphoma. 2000 Dec;1(3):226-31; discussion 232-3.
|
|
Autologous bone marrow transplantation after histologic transformation of indolent B cell malignancies. Biol Blood Marrow Transplant. 1999;5(4):262-8. PMID: 10465106 PubMed |
|
Rituximab-EPOCH - an Effective Salvage Regime for Relapsed, Refractory, or Transformed B-Cell Lymphoma. Results of a Phase II Study. Year: 2001 Abstract No: 1157 |
|
Treatment of Intermediate-and High-Grade Non-Hodgkin's Lymphoma U-M Comprehensive Cancer Center |
|
The Follicular Lymphoma International Prognostic Index (FLIPI) and the histological subtype are the most important factors to predict histological transformation in follicular lymphoma PDF
|
|
Revlimid (R) Demonstrates Activity against Relapsed/Refractory Aggressive NHL marketwatch.com
|
p53 mutations are associated with histologic transformation of follicular lymphoma. Blood. 1993 Oct 15;82(8):2289-95. PMID: 8400281 PubMed |
|
Transformation of follicular lymphoma to diffuse large-cell lymphoma: alternative patterns with increased or decreased expression of c-myc and its regulated genes. Proc Natl Acad Sci U S A. 2002 Jun 25;99(13):8886-91. PMID: 12077300 PubMed | PDF |
A: Yes. But it's a little bit different. The equivalent for indolent lymphomas is that most of them have a tendency, some more than others, to undergo histological transformation to a more aggressive disease. So that reflects clonal evolution, where a clone that gets additional hits. Once these things become tumors or become lymphomas, they become independent of normal regulatory pathways. They have a higher tendency to accumulate and to survive additional hits. And so what happens over time is that when our normal cells get genetic hits, our cells have huge amounts of surveillance pathways to kill those cells. Those cells die. Otherwise, we would be popping up with tumors all the time.
Because our genetic code probably gets hit constantly. You know, our body fixes them or the cells commit suicide through the apoptotic pathway. Tumor cells have a much higher tendency of, number one, not transcribing their code correctly. And number two, not committing suicide when the hit happened. So when you have an indolent process, a chronic process, that you have for years and years and years, over time it's just natural that you're going to get clonal evolution. A clone that gets a hit that gives it a proliferative advantage. And something's going to pop up. And that's what happens in CLL when it undergoes a blastic transformation. In any of the lymphomas, they undergo a large cell transformation. www.cancer.gov
New: High-grade transformation in splenic marginal zone lymphoma with circulating villous lymphocytes: the site of transformation influences response to therapy and prognosis. Br J Haematol. 2008 Jul 30. PMID: 18671706 |
|
Progression to large B-cell lymphoma in splenic marginal zone lymphoma: a description of a series of 12 cases. Am J Surg Pathol. 2001 Oct;25(10):1268-76. PMID: 11688461 PubMed |
|
Primary digestive Richter's syndrome. Mod Pathol. 2001 May;14(5):452-7. PMID: 11353056 PubMed | More |
|
Histological grading with clinical relevance in gastric mucosa-associated lymphoid tissue (MALT) lymphoma. Recent Results Cancer Res. 2000;156:27-32. Review. PMID: 10802860 | Related articles |